



Sex disparity in cardiovascular health
Important sex differences exist in CVD risk and risk factors. The rates of CVD, particularly ischemic heart disease (IHD), are significantly higher among men compared to women across different age groups, whilst women are more likely to have stroke or heart failure as their first event, particularly after age 70 [1].
There are various potential reasons behind this sex disparity [2, 3]. One possible explanation is that men tend to adopt more unhealthy lifestyles, including higher tobacco smoking rates, more consumption of red meat, and lower intake of vegetables, compared to women [2]. However, research that takes into account these unhealthy behaviors has shown that lifestyle factors may contribute to the difference, but they cannot fully explain it. Other hypotheses, such as differences in social support and physical activity between the sexes, also fail to provide a comprehensive answer [2].
Sex hormones have long been considered as a possible explanation for the lower cardiovascular mortality women have [4]. From a life course perspective, major cardiovascular risk factors such as lower levels of high-density lipoprotein (HDL)-cholesterol and higher systolic blood pressure (SBP) in men compared to women start to emerge during adolescence [5], indicating that sex hormones during puberty may play a role in adult health. For many years, the substantially higher mortality rate from IHD in men compared to women was attributed to women being protected by estrogen [6], rather than men being vulnerable because of some aspect of maleness. This could be due to the norms in the selection of potential causes for study in population health [7]. The possibility of protection against CVD and IHD from estrogen is consistent with the fact that the sex difference in CVD and IHD mortality narrows after menopause in women [4] and with the meta-analysis of observational studies of estrogen administration to women [8]. However, it is contradictory to the evidence from the Coronary Drug Project trial of estrogen administration to men in the 1970s, where the estrogen arms were stopped early [9]. After millions of post-menopausal women had been taking estrogens for years, Nancy Krieger’s paper from 2005 randomized controlled trials (RCTs) of estrogen administration showed that estrogen increased breast cancer and had no cardiovascular benefit for women [6, 10]. An alternative hypothesis is the “deleterious effect of maleness” [4]. Notably, men with Klinefelter’s syndrome have lower testosterone levels throughout their lives and a lower mortality rate from IHD than other men [11]. Legally castrated men also have a relatively lower rate of IHD [11].
More than a decade after the Women’s Health Initiative (WHI) trial showed that estrogen does not protect women against IHD or mortality [10], the role of hormones in women still attracts a lot of attention. Hormone replacement therapies have advanced rapidly over the past two decades. Early use of low-dose E2 during menopause seems to be favorable for women’s cardiovascular health [12] and contributes to a reduction in overall mortality. Furthermore, post hoc analyses from the WHI with extended follow-up indicate that younger participants (under 60) on estrogen alone had a decreased risk of cardiovascular disease outcomes [13]. The alternative candidate, sex hormones in men, got attention in recent years. For example, several Mendelian randomization studies showed that genetically predicted testosterone increased the risk of cardiovascular disease in men but not in women [14, 15], whilst sex hormone binding globulin lowered the risk of IHD, especially in men [16]. There is also evidence emphasizing the importance of sex hormone ratios. Evidence from a cohort study suggests that a higher estrogen to testosterone (O/T) ratio is associated with a lower risk of MI, while a higher free androgen index (FAI) correlates with a higher risk of MI after accounting for cardiovascular risk factors in men, but not in women [17]. More studies are needed to elucidate the underlying pathways and to explore more biomarkers explaining the sex difference.
Notably, although men have a higher risk of cardiovascular mortality, women have more severe symptoms [1]. For example, although both men and women with myocardial infarction (MI) are likely to present with chest pain, women may be more likely to have additional symptoms, such as epigastric discomfort, nausea, dyspnea, and fatigue [1]. The burden of CVD associated with metabolic conditions, particularly diabetes mellitus, is disproportionately higher in women than in men, a disparity that may be partly explained by differences in treatment that favors men [18]. Women often experience heart disease in a different way compared to men, and the lack of recognition of this has been shown to have adverse consequences [19]. Clinical trials in CVD primarily recruit men, despite it being well recognized that some drugs act differently in women and men [19].
There are several reasons behind this. From the cultural perspective, in various cultures, women may face limited access to healthcare resources due to financial dependency or societal restrictions, significantly affecting early detection and treatment of health conditions. In healthcare, both in primary and secondary prevention, there is evidence that women are undertreated, compared to men [19, 20]. Traditional norms in some communities often prioritize men’s health over women’s. In patriarchal societies, financial and decision-making power is frequently held by male family members, reducing women’s autonomy in healthcare decisions [21]. Consequently, this can lead to delays or barriers in seeking medical attention for cardiovascular symptoms, potentially compromising women’s health outcomes.
Traditional roles, such as caregiving for children, elderly parents, or other family members, along with domestic responsibilities and cultural norms, can significantly limit women’s ability to pursue healthy lifestyles, engage in physical activity, and practice self-care [20]. These roles are deeply ingrained and often lead women to prioritize socially expected duties over their own health needs. This pattern persists across various socioeconomic groups, where the demands of caregiving and domestic responsibilities can reduce the likelihood of women seeking timely and specialized medical care [22].
The impact of these roles has been further illuminated by the COVID-19 pandemic, which has exacerbated the pressures on women globally. The crisis has underscored how socioeconomic status and cultural expectations profoundly affect women’s physical and mental health. The increased burden of caregiving during the pandemic has amplified stress levels [23], reduced access to healthcare resources [24], and restricted opportunities for physical activity [25], further compromising women’s health and wellbeing.
Addressing these entrenched roles and expectations is critical for empowering women to embrace their health as a priority. By fostering environments that support equitable caregiving responsibilities and promoting societal shifts towards shared domestic duties, we can encourage women to seek the healthcare they need and deserve, ultimately enhancing their overall quality of life.
Many risk prediction models neglect to conduct sex-specific analyses, overlooking important sex-specific factors unique to women, such as female-specific metabolic/reproductive risk factors (parity and reproductive history, polycystic ovary syndrome (PCOS), pregnancy complications, menopause), as well as some established risk factors that differ in prevalence from those experienced by men, such as hypertension, diabetes, or smoking habits [20]. Similarly, diagnostic and treatment protocols often fail to consider sex-specific risk factors, leading to women being diagnosed or treated based on criteria calibrated for men. Despite well-established sex-specific symptoms of cardiovascular disease, these differences are frequently overlooked in research and clinical practice [26].
While significant efforts have been made to raise awareness over the past two decades [27], discussions about incorporating sex-specific statistical methods persist, largely due to the assumption that risk factors are universally shared across men and women. Even in the prediction models specifically for women, there is a lack of inclusion of female-specific predictors. Baart et al. [28] conducted a systematic review of 285 prediction models for women, including 160 female-specific models (designed exclusively for women). Surprisingly, despite the substantial number of models reviewed, only two of the 160 female-specific models (1.3%) included female-specific predictors [29].
Several studies have explored the added value of female-specific factors, such as pregnancy-related conditions, in cardiovascular risk prediction models, but the findings are inconsistent and inconclusive. For example, in the systematic review by Tschiderer et al. [30], which included nine models specifically examining the inclusion of sex-specific factors in existing risk scores, only slight improvements in risk discrimination were shown with the addition of factors like pre-eclampsia or age at first birth. Another study in a population-based retrospective cohort of women aged 15 to 49 who had been pregnant also showed that the prediction model with and without pregnancy factors had similar predictive performance, but the former had better clinical utility [31].
On the other hand, evidence also supports that the incorporation of sex-specific factors can enhance the accuracy of cardiovascular risk scores. In a population-based cohort study conducted by Naz et al. [32] in 4013 patients, they demonstrated that augmenting the Framingham risk score with pregnancy outcomes led to an improvement in CVD risk prediction, characterized by a higher C-statistic, which indicates enhanced discrimination, along with a modest enhancement in discrimination.
Pinpointing the root cause of such disparate findings is crucial. For instance, the majority of studies have predominantly targeted women aged 40 and above, overlooking younger women in their childbearing years or those who are pregnant. These populations, often deemed vulnerable, have historically received insufficient attention in research endeavors. Future research should target these groups to better assess the impact of female-specific predictors of cardiovascular risk in order to better identify what factors should be included in sex-specific prediction models, which could be useful in clinical practice.
Another critical concern arises from the development of new proprietary AI models built on biased prior knowledge that underrepresents women and minorities. Only by creating sex-specific prediction models from real-world studies can we lay the groundwork for AI-driven predictions capable of automatically stratifying patients’ risks and determining the most suitable management strategies. This also entails advocating for gender equality within the field of medical statistics in cardiology, encouraging statistical modeling that can account for distinctions rather than merely incorporating sex as a risk factor in the prediction models.
The sex difference not only exists in the CVD risk and risk factors, but also exists in the response to prevention and treatment strategies. For example, women have a 1.5- to 1.7-fold greater risk than men of developing adverse drug reactions [1]. The National Institutes of Health (NIH) is also calling for the consideration of sex differences in clinical trials [33], including women and minorities in clinical trials. Given the under-research on cardiovascular health in women, the Lancet women and cardiovascular disease Commission also calls for prioritizing sex-specific research on heart disease in women and intervention strategies for women [20].
The therapeutic effects and risk profiles of medications may be due to the sex differences in drug absorption, distribution, metabolism, and elimination [34]. The sex-specific effects may also be due to the interaction of medication and sex hormones. For example, statins, which lowered testosterone [35], have shown larger effects in lowering the risk of IHD in men than in women [14]. A similar sex-specific effect was also shown in nutrient supplements, such as berberine. Berberine is derived from traditional Chinese medicine and used as a nutrient supplement in the USA. Two recent systematic reviews and meta-analyses have shown that berberine may have a larger lipid-lowering and glucose-lowering effect in women than in men [36, 37].
The sex difference also exists in response to dietary intake and the effect of dietary factors. For example, a large cohort study in UK Biobank shows that red meat is related to a higher risk of IHD mortality in men but not in women [38]. The metabolites related to red meat intake also differ in men and women. Specifically, the positive associations of unprocessed red meat consumption with branched-chain amino acids and several lipoproteins and the inverse association with glycine were stronger in women, while the positive associations with apolipoprotein A1, creatinine, and monounsaturated fatty acids were more obvious in men [39]. L-carnitine, a metabolite related to red meat metabolism and especially rich in red meat, also has an association with a higher risk of IHD in men but not in women [40]. Another example is linoleic acid, the commonly used omega-6 unsaturated fatty acid. A Mendelian randomization study shows that linoleic acid is related to a higher risk of IHD and a shorter lifespan in men but not in women [41].
Bridging the gap: leadership, representation, and the path to equity in cardiovascular medicine
While addressing biological sex differences in cardiovascular risk, symptoms, diagnosis, and treatment is essential to delivering effective and personalized care, these efforts alone are insufficient. Today, clinical cardiology and cardiovascular research remain largely male-dominated. For example, a report from the Medical Training Review Panel in Australia showed that women in cardiology advanced training only accounted for 22% in 2018, and this proportion has not changed over the past nine years [42]. Achieving true equity in cardiovascular research and health outcomes also requires a structural transformation in who leads, designs, and delivers healthcare.
Sex disparities in academic and leadership roles
Despite decades of advocacy and the implementation of equity-promoting initiatives by governmental agencies and professional organizations, the academic and clinical environments still fail to effectively support women within the field [43]. Although recent data from the Association of American Medical Colleges show increased enrollment of women in medical schools and residency programs, women remain underrepresented in key leadership roles and as principal investigators in cardiovascular research [44]. They are less likely to secure senior faculty positions, receive fewer speaking invitations at major conferences, and are at a disadvantage in research visibility and funding, with female principal investigators receiving smaller NIH grant amounts than their male counterparts [45,46,47]. Women are also underrepresented among editors in chief of leading medical journals [48].
A major contributing factor is the persistent lack of institutional support for work-life integration. Societal expectations continue to place the responsibilities of family care primarily on women [20], leading to disproportionate challenges in managing both professional and personal roles. Parenthood, in particular, has been shown to negatively affect career progression for women, while having little to no impact on men’s academic trajectories [49].
Authorship and influence: the visibility challenge
In academic cardiology, publication productivity directly impacts promotion and recognition. However, women remain significantly underrepresented across authorship roles in major cardiology journals, a trend that has seen little change over the past decade [50]. Regional disparities exist, but in most regions, there are more publications with women as first author than as last author, the senior author (Fig. 1). Leadership roles in clinical trials exhibit the same pattern: only 10.1% of trial leadership committees included women, and over half (55.5%) had no female representation at all [51].

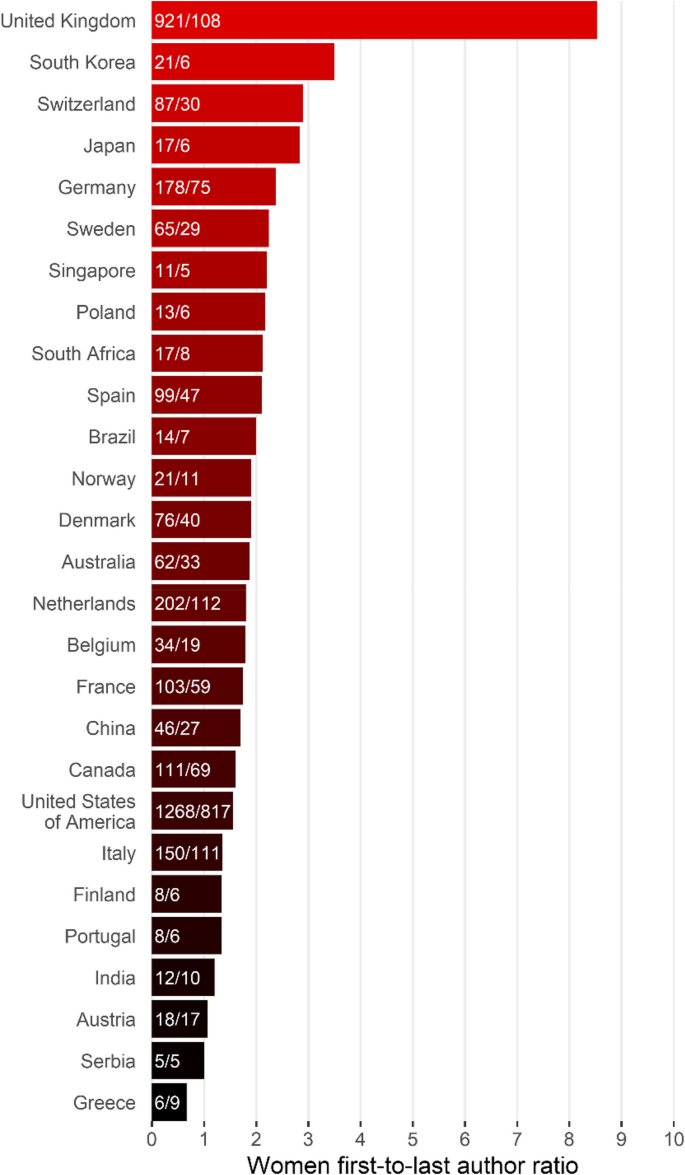
Geographic variations in the ratio of women as first and last authors. The statistics reported in the figure were calculated using the data from “Ridhima Goel, Samantha Sartori et al., Geographical Mapping of Gender Disparities in Authorship of Cardiovascular Literature. JACC. https://doi.org/10.1016/j.jacc.2024.03.427”
This underrepresentation does not only influence academic careers; it also has ripple effects in the research itself. Female researchers are more likely to engage and enroll other women in clinical trials [52, 53], so their absence from leadership reduces the likelihood of inclusive study designs and participant representation. This, in turn, limits the generalizability of findings and contributes to the continued underappreciation of sex-specific insights in cardiovascular research.
link