



Participants
Table 1 provides details of the participants’ backgrounds, which helped contextualise their responses, and informed interpretation.
Throughout the article, pseudonyms have been used to ensure anonymity
Group experiential themes
From the PETs, three Group Experiential Themes (GETs) with seven sub-themes were created (included in Fig. 1 below).

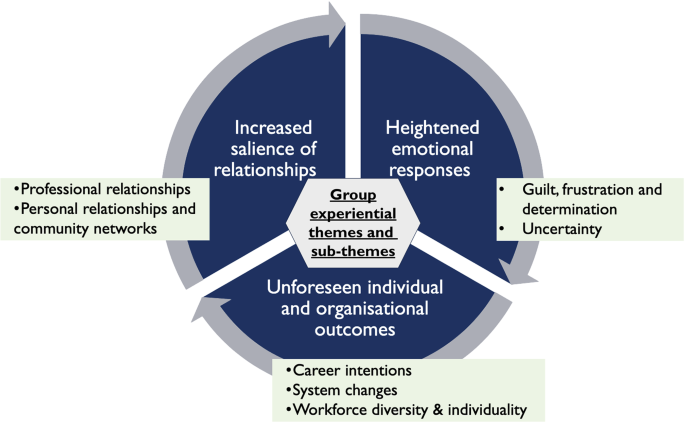
Group experiential themes and sub-themes
The extent of GPT experiences was illustrated by Ben who referred to death during COVID-19 being on an ‘industrial scale’. The cross-cutting themes discovered related to the heightened emotional responses, increased salience of relationships and unforeseen individual and organisational outcomes.
‘During a pandemic, it’s well, it’s almost like death on an industrial scale… the fact that it’s [death] just so much more common and being done in a very different way, it’s almost like it feels a bit more matter of fact now, just, in general and I don’t think it should.’ Ben.
Heightened emotional responses
The rapidly changing context of COVID-19 medical management, the rising death toll and novel challenges led to a variety of amplified, intense emotional response compared to pre-pandemic dying and death experiences.
Guilt, frustration and determination
Olivia, Rosie, Abeo, and Ben felt that the restrictions of COVID-19 impacted on every part of end-of-life care and support, with fewer hospice beds, GP home visits and hospital specialist reviews. This led to feelings of guilt and frustration as it did not meet what they saw as being a standard of good care. These emotions can be defined as moral distress (psychological unease when professionals cannot take the morally correct action) and moral injury (sustained moral distress leading to guild and shame as well as betrayal and anger) [44]. However, Rosie was able to remind herself that despite the changed circumstances, the core of general practice was still there, meaning that she saw it was still possible to deliver good care to dying patients.
‘I guess [its a] surprise that… in some ways… we can still execute bog standard general practice during a pandemic and people can have as close as possible… the experience they want of death and dying at home and it hasn’t completely rocked and destroyed that.’ Rosie.
A bittersweet experience for Ben was dealing wholly remotely with a patient who later died as this had a powerful personal and professional impact on him. He felt guilty about not being able to care holistically for the patient and family as much as he normally would, whilst trying to detach to protect himself from the emotional dissonance. He felt valued by the family which was rewarding and made him determined to provide the best care for other dying patients going forward.
‘It’s certainly one of those one of those things that… [will] stick with me forever… I diagnosed a chap was dying over the telephone and never actually saw him… it was upsetting personally, but also a little bit rewarding… because the family was so appreciative.’ Ben.
Uncertainty
The challenges around how to care for dying patients were entwined with general uncertainties about medical care. Unfortunately, three of the participants had worked with staff-members who had died from COVID-19. Participants had the added dimension of transmission risk to consider, mostly for patients, but also for themselves. This caused some anxiety and influenced their decision making, for example whether it would be safe to complete a home visit. They felt an internal emotional conflict of how to support vulnerable patients safely, whilst protecting themselves.
“What we were supposed to do in that circumstance? We didn’t feel that we really had any other option… I find it really difficult because I feel forced to be more distant from patients and from their family.” Olivia.
Julia and Abeo discussed their ethnicity being linked to an increased morbidity and mortality risk.
‘It was scary… this GP [who died from COVID-19]… I could just see myself in her shoes… children, young, no medical conditions and… from BAME* background as well… it does drum home that message, that this is real, and you have to be careful… it was scary for… myself and [my] family.’ Julia.
“Forty-four…. doctors died and only one was white, the other[s were] within the BAME* group… it terrified me. I just know that I’m in danger.” Abeo.
* Julia and Abeo used the term ‘BAME’ (Black, Asian and minority ethnic), which was widely used at the time of the interview but is not the preferred term now.
One of Julia’s frail care home patients was transferred to the emergency department due to the carer’s uncertainty about how to care for dying patients with COVID-19. The patient was not in his familiar environment, despite this being his preference, in his final hours of life. This situation demonstrates the intricacies of pervasive uncertainty when managing dying and death in a COVID-19 pandemic context.
Increased salience of relationships
Participants found different relationships offered support and comfort.
Professional relationships
Most participants had experienced positive teamworking and solidarity despite some isolating factors within GP surgeries, such as having to work alone or work from home, as well as the community-wide social distancing and lockdown measures. They found in-house and regional teaching and debriefing sessions to be a useful forum to share COVID-19 -related experiences and emotions of dying, as well as other unrelated subjects.
Three participants had felt isolated in their role and felt unable to discuss patients and those who were dying with their team easily. Olivia felt the loss of the usual connections with the practice staff due to a deliberate strategy to limit staff interactions to reduce spread of possible infection.
‘I feel like I had very little kind of connection to the nursing staff or the admin[istration] staff….we’re encouraged not to have much contact with them…. [we can’t] just go and chat with them… it’s sometimes difficult to, to have that sense of teamwork.’ Olivia.
Marie, who was shielding due to pregnancy and working from home, described a similar sense of isolation that resulted from the lack of direct in-person contact with colleagues. This was more challenging when having emotive conversations with dying patients and not being able to debrief or have a lighthearted chat with a GP team who understand.
Ben explained how he occasionally used alcohol to express his emotions when he was not able to reflect on some of his experiences because of cancelled teaching or supervision sessions.
‘Obviously in an anonymised fashion… [I] have a chat about [the patient] with my partner [about] anything that is particularly bothering me or it ends up coming out when i’ve had a bit too much to drink.’ Ben.
Olivia’s, Marie’s and Ben’s experiences show the importance of ‘normal’ professional contacts and emphasises the value of teaching sessions. When there was a lack of professional connection, GPT support needs were not always met and that lead to some GPT not coping well or struggling to process difficult experiences of dying.
Personal relationships and community networks
Several participants talked about the importance of the emotional support they received from loved ones, who provided advice, and the physical and emotional time and space to offload their feelings.
However, the pandemic had a personal impact on Julia, Abeo and Ben, who lost friends and relatives during the COVID-19 pandemic. The parallel of caring for dying patients professionally and experiencing death personally meant they discussed feeling complex emotions including anger, frustration and sadness.
‘Grieving for friends or family… it’s harder… than [grieving for] patient[s]… when friendship [or] blood is involved, it… drives it home… and [you] see yourself grieving over years.’ Abeo.
On a wider scale, the GPT were grateful for practical support beyond the GP surgery, for example, the local fire service and schools provided practical help to supply PPE as well as messages of encouragement and motivation.
Unforeseen individual and organisational outcomes
COVID-19 dying and death experiences made participants think more openly about their future careers and there were unforeseen individual and organisational changes within the healthcare system.
Career intentions
The pandemic directly influenced three GPT career decisions mostly positively with some negatives. Rosie’s had considered leaving GP training to apply for palliative care specialty training prior to COVID-19 pandemic however, her experiences of caring for dying patients reignited her passion for GP-led palliative care.
‘I kind of I started the job partly thinking about… leaving the GP programme to do palliative care training. And I think… [COVID-19 pandemic] made me want to be a GP who can do palliative care well… it’s better suited to what i want to do.’ Rosie.
Olivia had been considering whether a career in General Practice could work for her family life or if an alternative career would be better, however she felt that COVID-19 introduced new opportunities in technology and innovation in GP surgeries. Changes such as remote consulting and more flexible working, compared to pre-pandemic helped her visualise working as a GP in different roles, for example, telephone consulting and out of hours work which includes urgent care for dying patients in the community.
‘The job and the way that I’m working now bears no resemblance to… when I applied to become a GP all those years ago… that has definitely kind of raised lots of questions about what kind of work do…’ Olivia.
Kim had planned a six month ‘out of programme’ career break but as she was unable to travel during COVID-19 pandemic, Kim re-joined training as a second year GP registrar. Kim and her GP surgery experienced high numbers of COVID-19 deaths. It was a challenging time but she felt every experience of dying “teaches you… something new, something different”, which she wanted to learn from, to give patients and families a better experience of dying and death when she is a qualified GP.
System changes
Some of the GPT reflected on the multiple clinical and legal updates, and changes in guidelines and processes as a result of the COVID-19 pandemic, such as changes in death certification. At times, the GPT found it overwhelming and impossible to keep up to date with the daily, weekly, monthly changes and regular inconsistencies. There were, however, some benefits as there was less administration which freed up time to focus on clinical and caring responsibilities, such as calling bereaved family members. Some changes streamlined processes that has been undisputed medical standards for decades, e.g. online coroner referrals, prescribing anticipatory medicines over the telephone. Some GP trainees questioned why a it took a COVID-19 pandemic to implement essential changes to modernise some of the day-to-day GP medical practices.
‘The situation, the death certificate was a bit more straightforward because usually you already know this patient… the family, you know there are no concerns, and you go there and just see the body… it’s just so much time, energy and paperwork… [when] there’s no concerns… but nobody ever questioned it before COVID-19 happened.’ Julia.
Workforce diversity and individuality
An individual and organisational outcome from the COVID-19 pandemic for GPT has been the recognition that people from an ethnic minority have been disproportionally affected by the COVID-19 pandemic in many ways, including number of deaths. Julia felt valued as a staff member and felt nationally there was a positive move towards valuing diversity, especially in healthcare as more research and individual risk assessments were carried out with staff roles being amended if higher risks of morbidity and mortality were identified. The participants felt the NHS appeared to work together to value and support staff as individuals by reviewing those who possibly needed workplace adaptions e.g. ‘shielding’ pregnant staff like Marie.
Abeo and Julia had occupational health plans to reduce exposure and risk of COVID-19, however, at times the implementation of this was inconsistent, with community home visits being booked for them to high risk patients with respiratory symptoms when personal protective equipment was not available.
‘When it is [a] grey [area]… it’s unclear and people push the boundaries… but I just took the precautions, and you try your best.’ Julia.
link