



Study design and participants
In the current study, we performed a secondary analysis of data from a prospective multicenter cohort study of patients with advanced cancer [Clinical Trial Registry (ClinicalTrials.gov); Clinical Trial Number: NCT03222258; Study Registration Dates (First submitted: 2017-06-05; First submitted following the QC criteria: 2017-07-16; First Posted: 2017-07-19)]. The study examined the potential associations among survival, curability beliefs, and depressive symptoms in patients with advanced cancer. Some of the results of the prospective cohort study related to the effect of prognostic awareness on quality of life in patients with advanced cancer were published recently22. The current study recruited participants who were aware of their cancer diagnosis from 13 tertiary hospitals in the Republic of Korea between 17 December 2016 and 17 August 2018. Four of the 13 hospitals in this study were ranked among the “World’s Best Specialized Hospitals, 2025” in oncology: Asan Medical Center (3rd), Seoul National University Hospital (8th), Seoul National University-Bundang Hospital (57th), and Chonnam National University-Hwasun Hospital (116th) (https://r.statista.com/en/healthcare/worlds-best-specialized-hospitals-2025/ranking/).
The inclusion criteria were as follows: (1) age ≥ 19 years; (2) diagnosis of stage IV advanced breast, colon, gastric, pancreatobiliary, lung, or liver cancer, or malignant hematologic neoplasm; (3) anti-cancer treatment that included ongoing standard chemotherapy, interrupted standard chemotherapy, ongoing advanced anti-cancer treatment (such as immunotherapy or clinical trials) following standard chemotherapy, or cessation of all anti-cancer therapy; and (4) oncologist-estimated survival of > 6 months at baseline. Patients with poor cognitive capacity, an inability to read or understand Korean, or an inability to complete the survey due to poor physical condition were excluded. All oncologists participating in this study as attending physicians are active members of the Korean Society of Medical Oncology (KSMO; and have comparable levels of clinical expertise. The study protocol was approved by the Institutional Review Board of Seoul National University College of Medicine and Hospital (approval no.: 1602-142-745). The study was performed in accordance with the 1975 Declaration of Helsinki and its 2013 amendment. Informed consent was obtained from all participants.
Measures: sociodemographic and physical health status
At baseline, demographic factors (age, sex, marital status, religion, and place of residence), socioeconomic status (monthly household income and educational achievement), physical health (primary tumor site, physical performance, type of cancer treatment, and number of metastatic sites), and mental health (depressive symptoms) were evaluated using self-administered questionnaires during face-to-face interviews at an outpatient or inpatient facility.
With regard to cancer-related physical health status, physical functioning in daily life was assessed using the Eastern Cooperative Oncology Group performance status (ECOG-PS) scale23. This scale categorizes functioning in daily life into six classes: fully active and able to carry out all pre-disease activities without restriction (0), restricted in physically strenuous activities but ambulatory and able to carry out light or sedentary work, such as light house work or office work (1), ambulatory and capable of all self-care but unable to carry out any work activities, with the patient spending > 50% of waking hours “up and about” (2), capable of only limited self-care, confined to bed or chair for > 50% of waking hours (3), completely disabled, unable to perform self-care, and totally confined to bed or chair (4), and death (5).
Cancer-related symptom burden was assessed using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative (EORTC QLQ-C15-PAL) scores24,25,26. The EORTC QLQ-C15-PAL includes 15 items covering seven symptom domains—fatigue, pain, dyspnea, insomnia, appetite loss, constipation, and nausea/vomiting—as well as three functional scales assessing quality of life, physical functioning, and emotional functioning26. Most items are rated on a 4-point Likert scale (1 = “not at all,” 2 = “a little,” 3 = “quite a bit,” 4 = “very much”), while overall quality of life is evaluated on a scale from 1 (very poor) to 7 (excellent)26. Ten sub-scores are calculated and linearly transformed to a 0–100 scale26,27. Higher scores on the symptom scales indicate greater symptom severity, whereas higher scores on the functional and overall quality of life scales reflect better health-related quality of life26,27.
Measures: curability belief, patient’s perceived life expectancy, and depression
Curability belief was assessed by asking patients, “Do you think your illness will be cured?”22,28 Response options included: (1) “my cancer will be cured,” (2) “my cancer may be cured if the treatment is successful,” (3) “my cancer cannot be cured but treatment will control it,” (4) “my cancer cannot be cured and additional treatment is unsuitable,” and (5) “not sure28.” Curability belief was indicated by responses 1 or 2 only.
Patient life expectancy was evaluated with the item, “How much longer do you think you might live?”28 Participants selected one of the following options: (1) “similar to a healthy person of my age,” (2) “more than a few years,” (3) “more than a few months,” (4) “within a few months,” or (5) “not sure.” For comparisons between groups (Table 1) and MGM analysis (Fig. 2), responses were reclassified into two categories: “ ≥ several years” (options 1 and 2) and “ ≤ several months” (options 3–5).
Depressive symptoms at baseline were measured using the Patient Health Questionnaire-9 (PHQ-9)29,30, a nine-item tool where total scores indicate depression severity: 0–4 (none), 5–9 (mild), 10–19 (moderate), and 20–27 (severe)29. In this study, comorbid depression was defined as a baseline PHQ-9 score of ≥ 1031.
Measures: patient survival at 1-year follow-up and end-of-life care metrics
Patient survival at 1 year from study enrollment and baseline measures were assessed through information collected from participants, families, and physicians. Follow-up was conducted by research assistants at 3, 6, and 12 months in inpatient or outpatient settings. For patients who did not survive the 1-year follow-up, end-of-life data, including place of death, was obtained from caregivers. If participants could not be reached, physicians were consulted to confirm survival status. Those unreachable were categorized as “unable to contact.”
Statistical analyses: survival analyses
Demographic, socioeconomic, physical health, and mental health parameters were compared between the subgroups with curability beliefs (n = 239) and without curability beliefs (n = 143) using t-test for continuous variables and the chi-square test for categorical variables (Table 1). Univariate Cox proportional hazards regression analyses were conducted to examine the associations between 1-year survival of patients with advanced cancer and factors such as demographics, socioeconomic status, primary tumor site, number of metastatic sites, type of cancer treatment, performance status, symptom burden, and depression (Table 2). Furthermore, multivariate Cox proportional hazards regression models of 1-year survival were used to examine associations between 1-year survival and curability beliefs, with adjustment for demographic and clinical variables that posed significant risks to 1-year survival, as identified in the univariate analyses (Fig. 1). Post hoc multivariate Cox proportional hazards regression models were utilized to compare the association between survival and curability beliefs in subgroups without (PHQ-9 total score < 10) and with (PHQ-9 total score ≥ 10) comorbid depression at baseline, after adjustment for demographic and clinical variables associated with significant risks to 1-year survival in the univariate analyses (Fig. 1). Kaplan–Meier survival curves for the curability beliefs-by-depression interaction in patients with advanced cancer (Fig. 1) were generated using the MatSurv function32 implemented in MATLAB software version R2022a ( Fitting of the Cox proportional hazards regression models, along with calculation of hazard ratios (HRs) and 95% confidence intervals (CIs), was performed using the coxph function included in the R package survival ( P-values < 0.05 were considered statistically significant.

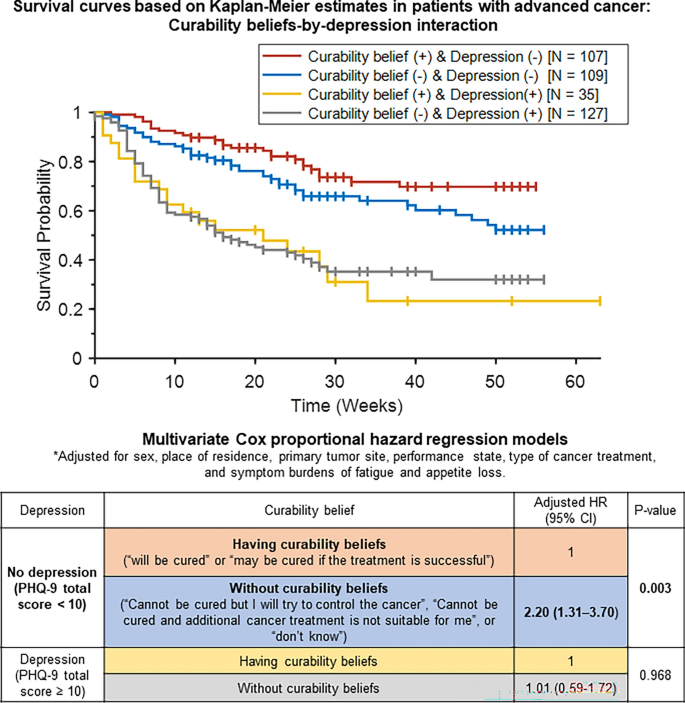
Interaction between curability beliefs and depression in survival probability. Upper panel shows survival probability plotted using Kaplan–Meier estimation. Lower panel displays the adjusted hazard ratio of not surviving 1 year, calculated through multivariate Cox proportional hazards regression. The model is adjusted for sex, place of residence, primary tumor site, performance status (ECOG-PS), cancer treatment type, and symptom burdens (EORTC QLQ-C15-PAL) of fatigue and appetite loss in patients diagnosed with advanced cancer. CI, confidence interval; ECOG-PS, Eastern Cooperative Oncology Group-Performance Status; HR, hazard ratio; PHQ-9, Patient Health Questionnaire-9.
Statistical analyses: MGM
To investigate associations among key clinical variables, we employed a MGM, focusing on 1-year survival (yes/no), curability belief (with/without), patient’s life expectancy (≥ years/ ≤ months), depression (PHQ-9 score ≥ 10/ < 10), primary tumor site (gastrointestinal-hepato-biliary-pancreatic/others), ongoing advanced anti-cancer treatment (including immunotherapy and clinical trials; yes/no), discontinued anti-cancer therapy (yes/no), performance status (ECOG-PS; 0–4), and symptom burdens of fatigue and appetite loss (EORTC QLQ-C15-PAL scores) in advanced cancer patients (Fig. 2). The MGM involved ten categorical, ordinal, and continuous variables33, where each variable was represented as a “node” and edges between nodes indicated undirected conditional dependencies or regularized partial correlations34,35,36. Two variables (i.e., nodes) were considered independent if they were not connected when conditioned on other variables37. To address potential spurious associations, we applied the least absolute shrinkage and selection operator (LASSO) method, which adjusted edge weights, setting smaller weights to zero, thereby reducing unnecessary connections38. For the MGM network derivation, we optimized edge weights through LASSO regularization (controlled by parameter λ) using a pairwise interaction model (k = 2) and the extended Bayesian information criterion (γ = 0)36. The strength of each association was represented by the thickness of the edges, with thicker edges signifying stronger associations39. To identify key nodes in the MGM network, we calculated betweenness centrality, which indicated the proportion of shortest paths passing through a given node, highlighting its importance in the network40. Additionally, “node predictability values” (displayed as pie charts41) provided insight into how well a node’s value can be predicted by the other connected nodes, comparable to R2 in regression analysis36,41,42. The MGM network was generated using the R package mgm43 and visualized through the Fruchterman-Reingold algorithm in the qgraph package39.

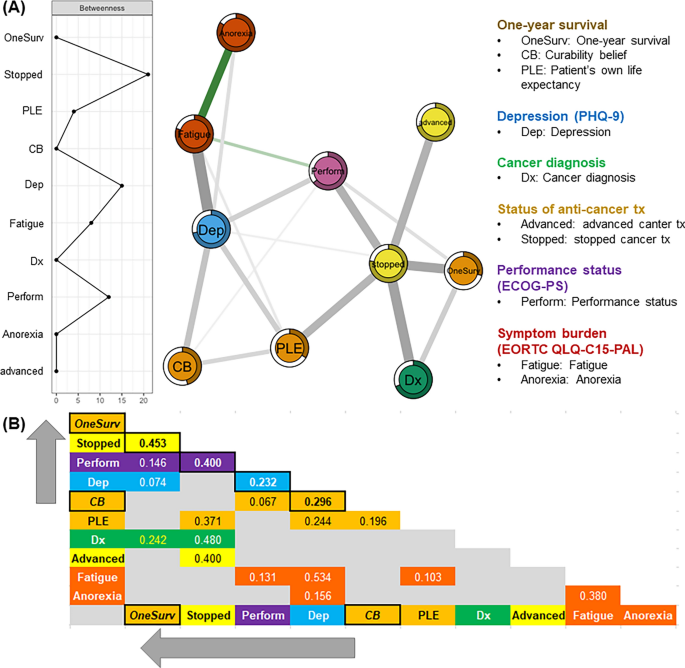
Mixed graphical model. Conditional joint probability distributions or regularized partial correlations of 1-year survival (Y/N), curability belief (“will be cured” or “may be cured if treatment is successful”: Y/N), patient’s perceived life expectancy (≥ years/ ≤ months), depression (PHQ-9; Y/N), cancer diagnosis (gastrointestinal-hepato-biliary-pancreatic/others), cancer treatment status [ongoing advanced anti-cancer therapy (Y/N), discontinued anti-cancer therapy (Y/N)], performance status (ECOG-PS; 0/1/2/3/4), and symptom burdens of fatigue and appetite loss (EORTC QLQ-C15-PAL) in patients with advanced cancer.
link