
Person-centred health care means ensuring that affected communities are leaders and partners in research

Studies show that people often do not have opportunities to engage in health-related decision-making with their health-care providers.
For people experiencing health issues and entering the health system as patients, an arrival at a hospital or a local clinic can be daunting. The health-care setting can be uncomfortable and unfamiliar. People may encounter challenges with communicating in a less familiar language or be faced with technical medical terms and jargon. There may be many health-care providers and their roles may not be clear to someone who comes into the health-care setting.
From the health-care providers’ perspective, new patients arrive every day, each with unique symptoms or conditions and personal circumstances. The support of patients as individuals is further complicated by underlying and systemic structural issues in health systems that can foster exclusion and oppression, including everyday racism. The outcomes can lead to medical mistrust and ultimately, poor care and health outcomes for patients.
People need support and opportunities to work with trusted health-care providers to make the best health decisions for themselves and their families. And those working within health systems need guidance and procedures to fully deliver on their key aspiration: the provision of person-centred care.
Person-centred care and shared decision-making
(Not Deciding Alone Team), Author provided (no reuse)
Person-centred care means treating people who face health issues as valued partners in health systems. The provision of care that is person-centred is much more than just treating symptoms or disease. People bring their own needs, values and perspectives that are vital to manage and improve their health.
Person-centred care upholds autonomy and has important benefits such as enhancing quality of care and patient and provider well-being, and may increase safety in health systems.
Health systems should be structured to support processes that are person-centred and ensure people have opportunities to acquire knowledge, skills and confidence to participate in their health care.
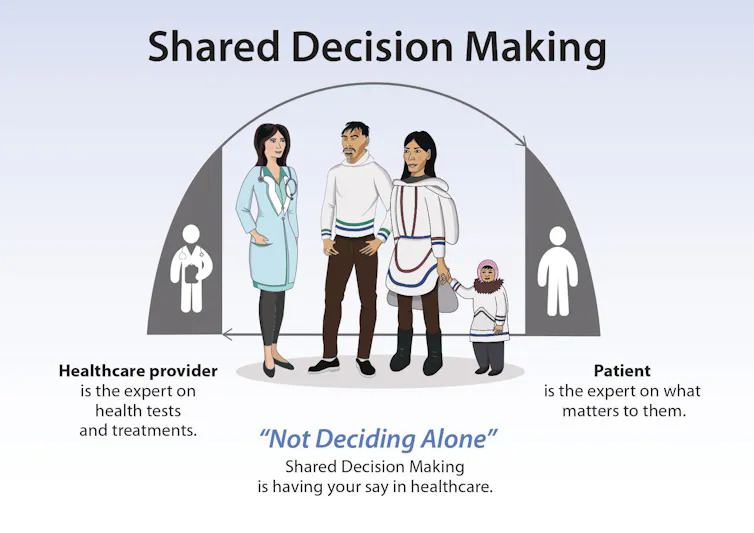
Person-centred care is not a given and can be a challenge to achieve without support for patients and health-care providers alike. Shared decision-making is one way forward to provide this support.

(Mackenzie Daybutch), Author provided (no reuse)
Shared decision-making is an evidence-based strategy that upholds person-centred care. It is a process that engages people with health-care providers to make decisions tailored to an individual patient’s needs, and based on the best available evidence, clinical expertise and patient-informed preferences.
Strategies to support shared decision-making have been shown to be safe and effective for general populations, and to offer even greater potential benefits to those who experience disadvantage in health systems.
Partnerships put people in the centre of health research
We are members of a team of service providers and academic researchers focused on person-centred care in health systems. Members of our team are part of the Inuit (Indigenous Peoples of circumpolar regions) or Indigenous community, and/or are of European heritage and work closely with the Inuit community. Together, we bring knowledge and experience with research, health systems and Indigenous cultures.

(Kimberly Fairman), Author provided (no reuse)
The delivery of person-centred care is a challenge. For example, health-care models often reflect values, knowledge systems, research and care practices that do not meet the needs of Indigenous people and communities. Research can contribute knowledge that can lead to societal change and opportunities for everyone to achieve optimal health and wellness.
Furthermore, research that is done in partnership fosters democratic processes of knowledge co-production. To attain health systems that support person centred-care, we need research that is done in ways that support the priorities and participation of the people the research is meant to benefit; in other words, research that is person-centred. We need to ensure that the people who use, or who are impacted by the research, can define the research and its outcomes as beneficial.
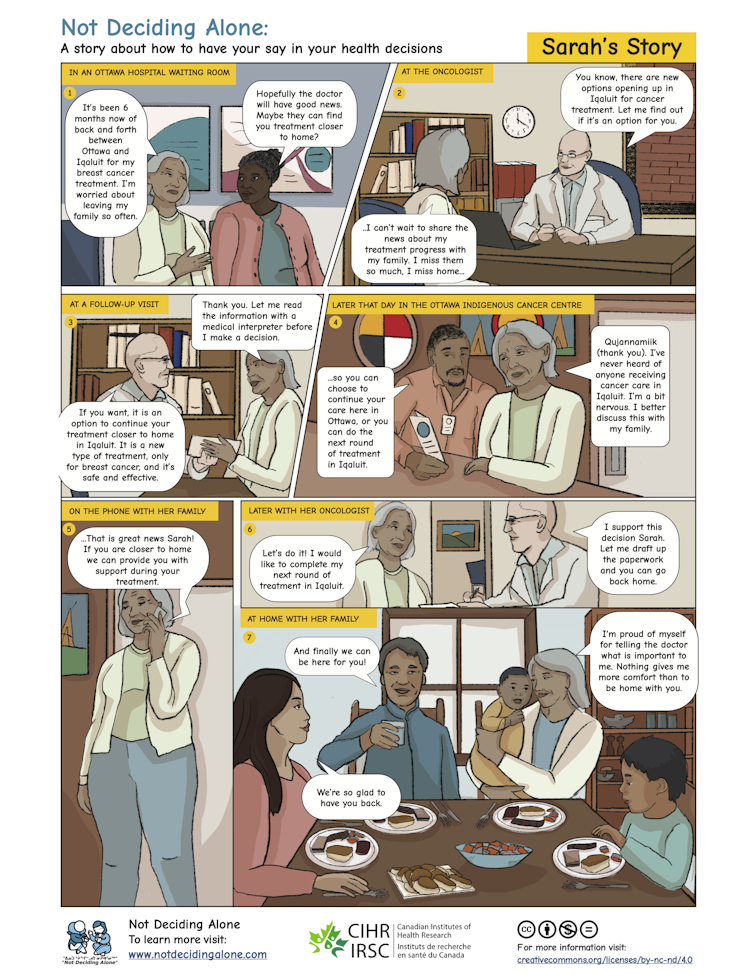
We have learned that while Inuit want to have their say in their health decisions, health systems and settings are not structured to support opportunities for their participation.
For example, Inuit who have a cancer diagnosis must navigate complex health systems and often face difficult decisions without support in unfamiliar and sometimes unwelcoming settings, far from home. Many factors adversely affect their participation in health decisions, including: the need to travel long distances for treatment; being separated from family and friends; and language and cultural barriers. Strategies to support shared decision-making are one way to mitigate these issues.
(Not Deciding Alone Team), CC BY-ND
Learning to put people in the centre of health care
We set out to learn from existing research about how Inuit and other Indigenous Peoples around the world can be supported in their health decision-making. We determined the scientific merit of the studies and how well they aligned with the principles of collaborative research with Indigenous Peoples.

(Not Deciding Alone Team), Author provided (no reuse)
We found that some of the study reports indicated they were led entirely by Indigenous scholars and/or communities, or included a mix of Indigenous people or communities with non-Indigenous academic researchers on the study teams. These studies were inclusive of Indigenous knowledges in the research. We referred to these studies as “Indigenous-oriented.”
Other studies did not report on leadership or inclusion of Indigenous partners and were based only on western academic knowledge. We referred to these studies as “western-oriented.”
While all the studies we found focused on the support of Indigenous Peoples in their health decision-making, only one group of studies supported person-centred care.
The Indigenous-oriented studies investigated strategies to change underlying and systemic structural issues in health systems, to make them more acceptable and aligned with the needs, values and perspectives of Indigenous groups. We found the Indigenous-oriented studies, with the leadership and partnerships of the people the research was intended to benefit, to be in support of person-centred care.
In contrast, the western-oriented studies took health promotion approaches to change peoples’ behaviours, outside of health settings and were less supportive of person-centred care.
Person-centred care through partnerships
Our work indicates that, in the field of Indigenous health, tackling the challenge of inequities and challenging underlying and systemic structural issues in health systems to support person-centred care is achievable through partnerships with people and communities who will use or be affected by the research findings. Our work also indicates there may be applicable lessons for working with other groups who may be at risk or experience disadvantage in health systems.
Not Deciding Alone, a team of Inuit-led and Inuit-specific organizations and academic health researchers who are active in health-care systems that provide services to communities in the Qikiqtaani region of Nunavut and in Ottawa, co-authored this article.
link




