



Study design
This study employs a non-equivalent control group, non-synchronized design to evaluate the effectiveness of a prenatal environmental health program for pregnant women, utilizing YouTube as a platform. This study adhered to the TREND (Transparent Reporting of Evaluations with Non-randomized Designs) reporting guidelines.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) pregnant women over the age of 20 and before 36 gestational weeks, (2) pregnant women who wished to participate in the antenatal education program at the public health center, and (3) pregnant women who attended all 4 weeks of pregnancy education. The exclusion criteria included: (1) pregnant women with pre-existing or current diseases, (2) pregnant women who did not understand Korean, and (3) pregnant women who did not possess a smart device to watch YouTube videos or attend Zoom meetings. Participants who did not complete all seven YouTube videos were considered drop-outs.
Allocation
Participants were selected using a purposive sampling method from individuals attending antenatal education programs at public health centers in C City, Gangwon Province, and G City, Chungcheong Province. Neither randomization nor blinding was performed. The researcher met with the directors of the public health centers and maternal centers to explain the study’s purpose, data collection period, research methods, and to obtain permission. Pregnant women attending the antenatal education program at the health center were asked for written consent to participate in the study. The purpose and methodology of the study were explained to them before the program began. Trained research assistants provided the study description and written consent form, allowing participants ample time to understand the study objectives and procedures. Questionnaires were distributed to those who voluntarily agreed to participate.
Intervention
The creation of the YouTube video adhered to the ADDIE (analysis, design, development, implementation, evaluation) process [12]. This process was documented in a protocol, and the experimental study protocol was registered with the Clinical Research Information Service of the National Institutes of Health, Centers for Disease Control and Prevention (KCT0007006).
Analysis phase
The researchers conducted a systematic review to search for YouTube videos related to women’s health, specifically focusing on environmental health. They found no such applications on YouTube. To locate relevant articles, they searched databases such as PubMed, Cochrane, CINAHL Complete, Embase, ERIC, and RISS, using the keywords “women’s health” and “YouTube.” The only pregnancy-related YouTube topics discovered were epidural anesthesia in obstetrics [6], sexuality in childbirth [1], and placenta accreta [7]. The researchers selected YouTube topics based on an internet-based systematic review of maternal environmental health and a study of maternal environmental health needs. They prioritized topics such as environmental hormones, chemicals, heavy metals, nutrition, fine dust, and emission methods, based on meetings among researchers and previous studies [13].
Design phase
The researchers created the content for the YouTube video education by developing a storyboard and producing an initial PowerPoint slide draft, which was divided into seven subtopics. These subtopics included endocrine disruptors and pregnancy, chemical exposure and pregnancy, heavy metal exposure and pregnancy, nutrition and pregnancy, fine dust exposure and pregnancy, environmental toxin release during pregnancy, and environmental toxin release during postpartum. To validate the content, the advisory team consulted with two professors of women’s health nursing and one midwife. They were asked two questions regarding the appropriateness and comprehensibility of the educational content, with responses given on a Likert scale ranging from 1 (very inappropriate and very difficult to understand) to 5 (very appropriate and very easy to understand). All responses were between 4 and 5 points, and the content was subsequently adopted.
Development phase
The researchers converted the PPT into a video lecture. Each video covered one of the seven topics and ranged in length from 6 min 35 s to 12 min 24 s, with a total duration of 1 h 22 min 35 s. The training materials included lectures, images, and animations. The videos were uploaded to a YouTube channel and made accessible exclusively to pregnant women who shared their YouTube addresses. One video was provided in the first week, followed by two videos each in weeks 2–4, resulting in a total of seven videos over the 4-week period (Table 1).
Implementation phase
The researcher recruited the experimental group from a public health center in City C, Gangwon Province, and provided four childbirth education sessions and YouTube videos through small group education via online Zoom meetings. The control group was recruited from a public health center in City G, Chungcheong Province, and was provided with four sessions of general in-person prenatal group education for pregnant women participating in childbirth education. The experimental group received the prenatal education program through videoconference in a Zoom room, totaling 8 h over 4 weeks, with 2 h per week, led by researchers and midwives in March, April, September, and October 2022. The program’s content included understanding pregnancy, pregnancy health management, understanding childbirth, pain control during childbirth, environmental risk factors during pregnancy, prenatal environmental health behavior, postnatal health management, breastfeeding, and baby care. Questions and answers were included after each session, and YouTube videos were made available through KakaoTalk (a social media platform widely used in Korea) following each session. A research assistant checked whether participants had watched the videos and, if not, encouraged them to participate via phone and text. For the control group, a face-to-face antenatal education program was delivered by a researcher for 2 h per week over 4 sessions in April, June, August, and October 2022, totaling 8 h in the health center training room. The control group program’s content consisted of prenatal healthcare on the first day, childbirth healthcare on the second day, postpartum healthcare on the third day, and newborn healthcare on the fourth day. The time was the same as the experimental group, and the control group was provided with YouTube videos after completing the education.
Evaluation phase
Pre-test: Prior to the first session, both the experimental and control groups were surveyed either online or in person. The pre-survey included a questionnaire that inquired about the participants’ general characteristics, obstetric features, social support, and environmental health behaviors, taking approximately 10–15 min to complete.
Post-test: The post-test took place in week 4, immediately after the conclusion of the antenatal education program. The content and methodology of the questionnaire were identical to those of the pre-test, but with the inclusion of questions regarding satisfaction with the educational content.
Assessments
Data collection took place from March 30 to November 2, 2022. The experimental group was assigned to a public health center in C City, Gangwon Province, while the control group was assigned to a public health center in G City, Chungcheong Province. Both the control and experimental groups underwent a pre-test at the beginning of their first prenatal education session and a post-test at the conclusion of their fourth session. For the experimental group, researchers conducted childbirth classes via a Zoom conference and provided YouTube videos for each session. In contrast, the control group’s childbirth classes were conducted in person. Upon completion of the post-test, the control group was provided with the YouTube video links. All participants received a gift at the end of the study.
Outcome measurements
Social support
The Perceived Social Support through Others Scale-8 (PSO-8) was utilized in this study [14]. The PSO-8 comprises three factors: 4 items related to the quality of care provided, 2 items addressing women’s personal attitudes, and 4 items concerning the experience of stress during labor. There are a total of 8 questions, with each question being answered on a 5-point Likert scale that ranges from 1 “not at all” to 5 “very much.” The overall score ranges from 8 to 40, with higher scores signifying greater social support. The internal consistency reliability, as measured by Cronbach’s alpha, was 0.91 for the original instrument and 0.95 for this study.
Environmental health behaviors
The environmental health behavior measure for women was adopted from a study by Kim & Kim [15]. This tool comprises 17 personal environmental health behaviors and 16 community environmental health behaviors. Personal environmental health behavior is divided into four factors: 7 lifestyle, 4 personal hygiene, 3 diet, and 3 dust-related behaviors. Community environmental health behaviors are also divided into four factors, with 5 reduction, 5 involvement, 3 recycling, and 3 reuse behaviors. The scale employs a 5-point Likert scale, ranging from 1 “not at all” to 5 “very much.” Total personal health behavior scores range from 17 to 85, while total community health behavior scores range from 16 to 80, with higher scores indicating higher levels of environmental health behavior. The internal consistency reliability, as measured by Cronbach’s alpha, was 0.90 for personal environmental health behavior and 0.91 for community environmental health behavior in the original instruments. In this study, the values were 0.85 and 0.87, respectively.
Content satisfaction
Content satisfaction was assessed using the e-learning satisfaction scale tool, which was designed to measure satisfaction in online education [16]. This tool comprises three factors: content (8 items), interface (5 items), and communication (4 items). For this study, only content satisfaction was considered. The scale utilizes a 5-point Likert scale, ranging from 1 (“not at all”) to 5 (“very much”). Total scores can range from 8 to 40, with higher scores indicating greater content satisfaction. The internal consistency reliability, as measured by Cronbach’s alpha, was 0.93 for the original instrument and 0.95 for this study.
Sample size
The number of participants was calculated using G*Power 3.1.9.4 [17]. A two-tailed independent t-test was specified with a significance level of 0.05, a statistical power of 0.90, and an allocation ratio of 1:1. The target effect size was set to d = 0.80, which corresponds to a medium-to-large magnitude and was adopted from a prior experimental study involving a YouTube application [1]. Based on these assumptions, the required total sample size was estimated at 70 (35 per group). To accommodate an anticipated 20% dropout rate, the recruitment target was set at 84 participants (42 per group). Ultimately, in the control group, 8 participants did not attend the training, resulting in 34 participants included in the analysis. In the experimental group, 4 participants were excluded due to insufficient responses to the questionnaire, leaving 38 participants for the final analysis (Fig. 2).

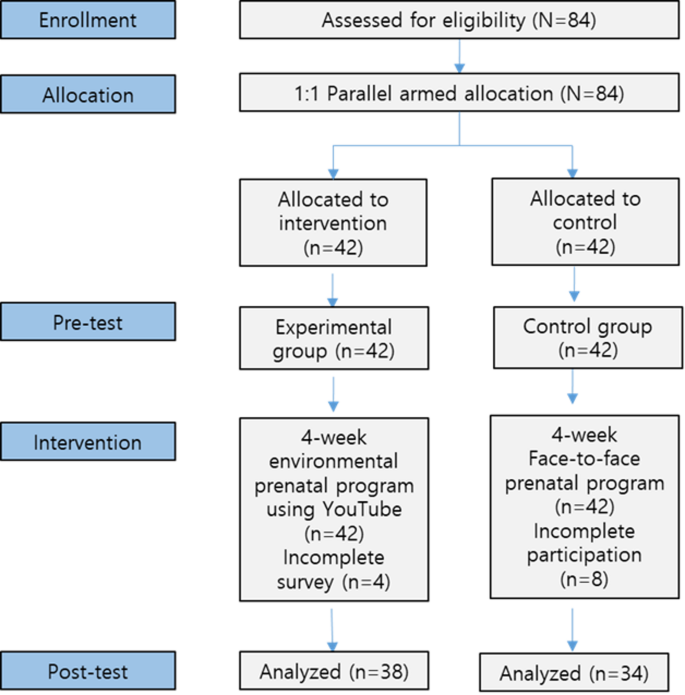
Flow diagram of the research process
Ethical consideration
This study received approval from the Institutional Review Board of the researcher’s university (KNU-IRB-2021-113). After obtaining permission from the directors of the health center and the maternal and child health center, the researcher personally conducted the survey. To safeguard the rights of the participants, the study’s purpose and methodology, the potential benefits and drawbacks of participation, privacy and confidentiality, and the option to refuse or withdraw were explained prior to data collection, and consent was obtained. Participants in the face-to-face training were interviewed in person at the health center training room, following quarantine measures and signing the instructions and consent form. Those participating in the Zoom meetings confirmed their intention to participate via text and phone, and completed the survey using an online Naver form.
Statistical analysis
The collected data were analyzed using the SPSS/WIN 26.0 program. The general characteristics, obstetric characteristics, social support, satisfaction, and environmental health behaviors of the subjects were analyzed by frequency, percentage, mean, and standard deviation. To test for homogeneity between the control and experimental groups in terms of general characteristics, obstetric characteristics, social support, and environmental health behaviors, we conducted the t-test, Mann-Whitney test, and chi-square test after assessing normality. The normality of the dependent variable was evaluated using the Shapiro-Wilk test, and the differences in post-hoc scores between the control and experimental groups were examined using the t-test and the Mann-Whitney test.
link