
Addressing healthcare inequalities in prisons: the vital role of nursing

Find out how nurses can address the health inequalities experienced by people in prison and promote equitable care in this third article in a series on stigmas in healthcare. This is a Journal Club article and comes with a handout that you can download and distribute for a journal club discussion.
The NT Journal Club offers an opportunity to reflect on practice, share insights and ideas in a relaxed and sociable setting, and gain participatory CPD hours towards revalidation. Click here to find out about the NT Journal Club and for more journal club articles to discuss.
Abstract
This article – the third in a series on stigmas in healthcare – explores the key factors contributing to health inequalities in UK prisons, including environmental constraints, communication barriers, staffing issues and the reactive nature of care in this setting. It highlights the diverse health needs of the prison population, including those with learning disabilities, mental health illness or long-term conditions, and the role of nurses in promoting equitable, person-centred care. Strategies such as peer education, telehealth and trauma-informed practice are discussed as ways to enhance healthcare delivery. The article also calls for greater recognition of the specialist role of prison nurses, and improved education and support for staff working in custodial environments.
Citation: Guttridge H et al (2025) Addressing healthcare inequalities in prisons: the vital role of nursing. Nursing Times [online] 121: 9.
Author: Heather Guttridge, Oonagh McCloy and Shannon Porter are all lecturers at Queen’s University Belfast.
Introduction
Health inequalities are seen as the differences in the healthcare that people receive and the opportunities available to them that contribute to health, including access to services, health status and behavioural risks (Williams et al, 2022). Among those at risk of experiencing health inequalities are socially excluded groups of people, which includes the prison population and those of low socioeconomic status (Williams et al, 2022). This reinforces the concern raised by the House of Commons Health and Social Care Committee (2018), which asserted that “a prison sentence is a deprivation of someone’s liberty: it is not a sentence to poorer health or poorer health and care services”.
Multiple sources of stigma in prison settings can intensify effects on prisoners, which impact on their quality of life, mental health and access to parole programmes (Matheson et al, 2022). Addressing stigma is essential to enhance all aspects of healthcare in prisons. This includes reproductive healthcare for incarcerated women – a population that has risen 19% over the last 32 years (Prison Reform Trust, 2025) – and care for people with learning disabilities who are over-represented in prisons, making up approximately 30% of the prison population (Prison Reform Trust, 2023). According to Matheson et al (2022), people with learning disabilities are particularly vulnerable to health inequalities and:
- May not receive adequate help with daily living needs;
- May be more likely to be physically assaulted;
- May be more susceptible to illicit activities.
More than two-thirds of those with learning disabilities in prison have said they would not know what to do if they felt unwell (Matheson et al, 2022).
Guttridge et al (2024) stated that, although healthcare delivery in prisons had improved, it remained substandard. Further improvements are needed to provide healthcare to those who are incarcerated that is comparable to that which is expected by the general population.
Exploring the unique challenges to providing person-centred care in the prison setting highlights the complex interaction of factors that result in health inequalities. These factors include the diverse health needs of patients, environmental factors, a reactive and ad-hoc approach to care, and the role of the nurse as a care provider in a prison setting.
Health needs of prisoners
Throughout the UK prison system, healthcare inequalities are evident: there is a higher rate of mental health conditions and physical long-term conditions (LTCs) than in the general population, including higher rates of suicide and conditions such as diabetes and heart failure (Prison Reform Trust, 2023; Scottish Government, 2022). These challenges are compounded by an ever-increasing prison population and a corresponding decrease in staffing ratios (Ismail and de Viggiani, 2018).
A high proportion of prisoners are aged >60 years – a demographic linked with LTCs. An estimated 85% of prisoners in this age group are living with a major illness (Guttridge et al, 2024). Overall, the health needs of prisoners are complex and diverse; as a result, greater attention is needed to enhance prison health services and ensure they are on a par with those available to the wider population (Rippon et al, 2021).
Environmental factors
Environmental inequalities that affect health can begin from the moment a person enters prison. Wright et al (2021) stated that the health assessment and compulsory screening after sentencing should be completed by a registered nurse. This helps to identify current health concerns and LTCs that can be acted on appropriately. Both Wright et al (2021) and the National Institute for Health and Care Excellence (NICE) (2016) advocate for the use of health assessments on arrival to prison. However, the prison system does not need to adhere to these recommendations, which leads to inconsistences in care provision.
The completion of a health assessment gives the prisoner an opportunity to communicate their needs, discuss medications and report any LTCs. However, this process is reliant on what the prisoner discloses to the assessor; as such, distrust of the prison healthcare system may prevent them from being fully open, so opportunities for an honest health appraisal can be missed and the safety of the prisoner compromised (Vandergrift and Christopher, 2021).
Rippon et al (2021) suggested that a community-based handover would be more appropriate, which gives clear instructions on how known health conditions have been managed and a list of medications. This could contribute to a seamless handover of health needs and be more effective than completing an assessment in a stressful, and often unfamiliar, environment. Conducting an assessment on admission can result in medications being missed as the case study in Box 1 highlights.
Box 1. Case study after admission to prison
Background
43-year-old male
Past medical history: Epilepsy since childhood
Prison setting: Category C prison
Medications: Prolonged-release carbamazepine 400mg twice a day; multiple other medications [not specified] for drug and alcohol detoxification programme and smoking-cessation programme
Friday
07:00: Prisoner receives medication as part of daily routine
11.35: Arrives after transfer from category B prison
14.04: Healthcare screening is carried out by nurse. Nurse notes medication status as ‘not in possession’ and that prisoner has concerns about his epilepsy. ‘Urgent priority’ prescription request sent to doctors via computerised system
15:03: Second ‘urgent priority’ prescription request is sent
19:16: Prescription request completed remotely, but carbamazepine is not included. Evening dose of carbamazepine is missed
Saturday
08:13: Nurse advises doctor that prescription for epilepsy medication was missed the previous evening and is needed urgently
12:23: Doctor states prescription has been completed, which will need to be printed and signed on Monday. Carbamazepine is not stocked at the prison, so will need to be obtained with a standard prescription form from a local pharmacy
Sunday
15.01: Prisoner has two epileptic seizures in his cell: the first lasts approximately seven minutes, the second approximately two minutes. Nurse administers rectal diazepam
15:01-16:28: Emergency services are called. Ambulance crew arrives. Prisoner has two smaller seizures
16:28: Prisoner is taken to a local emergency department, where carbamazepine 400mg is administered
~19:40: Patient is transferred back to prison
Monday
17:30: Prisoner receives first dose of carbamazepine, which he then receives twice daily
Source: Extracted from: Health Services Safety Investigations Body (2019)
Rippon et al (2021) also noted the restrictions to fresh air and space in prison, which can act as obstacles to addressing health needs and adopting a healthy lifestyle. These can also impede the nurse’s ability to advocate effectively for their patients. Other contributing factors include:
- Lack of communication between staff;
- Lack of communication between staff and prisoners;
- Lockdowns (which can last for up to 23 hours);
- Solitary confinement, and a minimal amount of nutrition-based options.
Some prisons have initiatives to improve prisoner health, such as well-men and well-women clinics running alongside health champion schemes. These are prisoner focused and encourage individuals to seek treatment, but they are not available in all UK prisons. As a result, healthcare disparity between prison populations remains, leading to further healthcare inequalities in the prison system (NHS England, 2023).
Health promotion in prison settings
Nurses advocate health promotion, self-management and empowerment – all of which include the holistic needs of the patient and a patient-centred care model (Nursing and Midwifery Council (NMC), 2018). Rippon et al (2021) noted that, to implement the correct approach in the prison environment, suitable health models are needed to guide nursing practice and support the multidisciplinary team (MDT). Nonetheless, as the environment must prioritise safety for prisoners, the public and staff, engagement in health promotion activities can be difficult.
According to Avieli (2023), by default, the prison environment can be authoritarian and structured, which restricts the free-flowing nature of health promotion and limits self-management of LTCs and mental health. This can inhibit prisoners’ engagement in health promotion and contribute to widening the care gap. Furthermore, Avieli (2023) stated that the environment leads to a lack of motivation, reduced self-management and feelings of disempowerment; these difficulties, combined with the rigid prison routine, have little correlation with health-promotion activities for the general public.
As part of broader efforts to address healthcare inequalities, the NHS-commissioned Reconnect project focuses on care after custody, supporting the prisoner’s transition to community services after incarceration to maintain healthcare provision made while in prison (NHS England, no date).
“A prison sentence is a deprivation of someone’s liberty… not a sentence to poorer health or poorer health and care services”
Communication and the ad-hoc nature of care
Rippon et al (2021) found that poor communication in the MDT proved to be a problem in prison healthcare systems, and was especially heightened in mental health care. When focusing on physical health, Guttridge et al (2024) suggested that prisoners are sometimes not taken seriously when they raise concerns about their health, and do not receive the timely response they might expect if they were in the community.
The NMC acknowledged this issue and supports greater engagement and implementation of links between MDTs to enable effective communication (NMC, 2018). However, in the custodial environment, this can be difficult to navigate due to the ad-hoc nature of care and the myriad multidisciplinary agencies operating both within and outside of the prison, which can lead to a lack of clear infrastructure for healthcare delivery in the prison system (Toledanes et al, 2021).
The Ministry of Justice and HM Prison and Probation Service (2024) highlighted the need for better collaboration and communication between MDTs to ensure seamless delivery of care, reduce harm and prevent avoidable deaths. Communication delays can lead to disengagement, disparity and disempowerment for the prisoner, and these clear divides inhibit the prisoner’s healthcare experience (Wright et al, 2021).
Education and staffing levels
Discrepancies are evident in both staff education and staffing levels in the prison healthcare setting (Arif, 2018); there is a need for education to address the gaps in training related to specific diseases, such as dementia (Gaston et al, 2022).
Health safety was also highlighted in a 2022 report by the Prisons and Probation Ombudsman, which suggested that healthcare in prison was mainly provided on an emergency-only basis. Staff need education and knowledge of physical and mental deterioration to:
- Engage with early escalation and intervention;
- Reduce emergency care requirements.
The report further highlighted that refresher courses were often delayed due to staffing shortages, which raised concerns about potential knowledge gaps that could compromise prisoner safety.
Guttridge et al (2024) also emphasised the need for adequate training and education for prison staff, which not only empowers them to engage safely in potentially life-threatening situations, but also safeguards the health and wellbeing of prisoners. Arif (2018) noted that some prisons delivered comprehensive training packages, but these were often conducted remotely, as staff were not given time to complete them during working hours.
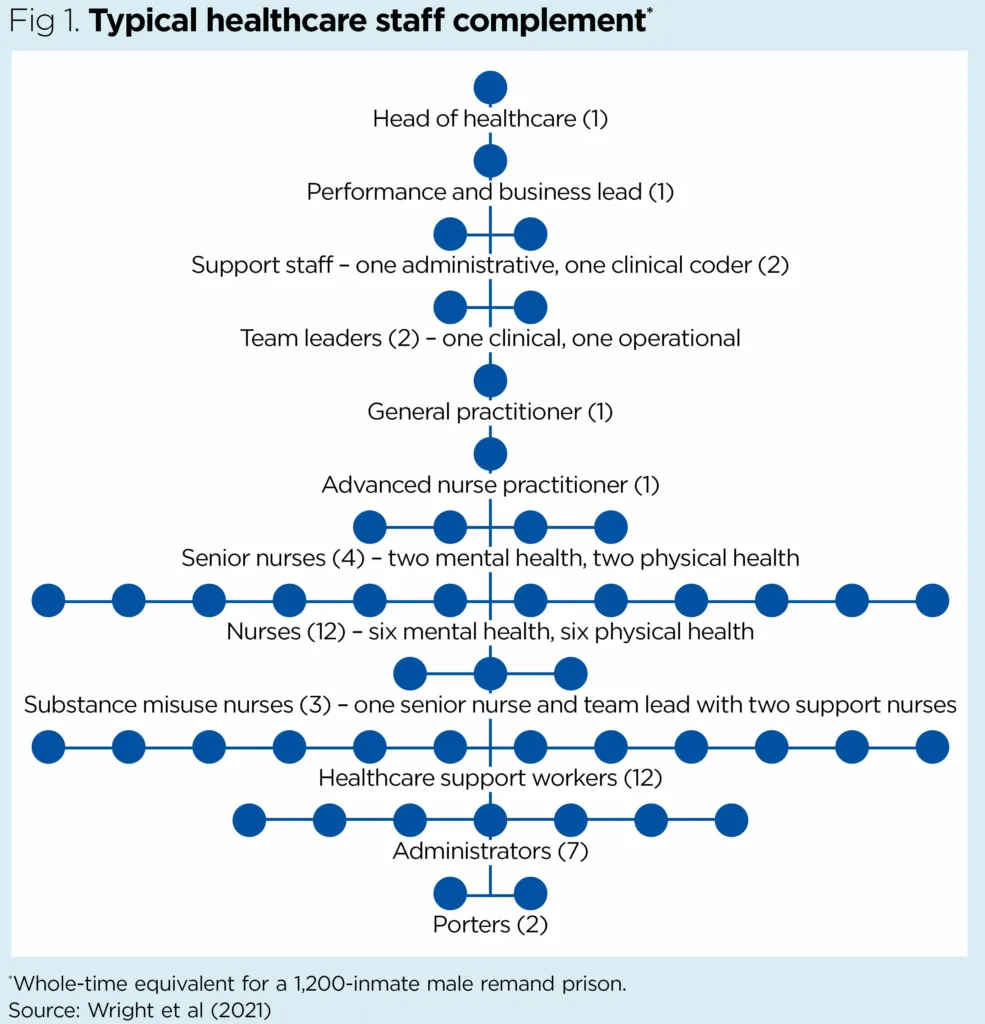
Fig 1 shows a typical staff complement in a remand prison with 1,200 inmates – although this can vary depending on the size and category of the prison. Wright et al (2021) further highlighted the need for specialist nurses in the judicial system. Goddard et al (2019) argued that the specialist role needs to be firmly linked with the professional identity of the prison nurse. This can be encouraged through training in an environment in which the nursing role conflicts with the prison regime and security protocols.
Toledanes et al (2021) cited safety as a concern, especially for prisoners with LTCs such as asthma, which is more prevalent in the prison population than the public. They delivered an educational intervention in a juvenile facility that encouraged staff to make sure inhalers were used correctly; this quality improvement programme showed a significant statistical decrease in asthmatic exacerbations. Taking this into consideration, it is evident that there are inequalities with the education received by staff in prisons throughout the UK.
Signs and symptoms of a potentially deteriorating prisoner can be missed or not recognised in a timely manner, potentially causing adverse effects, standardised and timely education and updates are needed for all prison staff and health professionals, so the provision of quality healthcare to all prisoners is in line with that available to the general population.
Ethical dilemmas and moral distress
There are many barriers in the prison environment that contribute both to health inequalities among prisoners and to the individual challenges faced by nurses working in that environment. It is important to acknowledge that nurses serve as primary caregivers in prisons and are the first point of contact for prisoners, ensuring access to healthcare services (Goddard et al, 2019). Goddard et al (2019) went on to discuss the frustrations felt by nurses when faced with obstacles to providing care in a prison environment: as an example, they noted that security requirements can limit the time spent providing care and can affect patient access to healthcare services.
Box 2 defines the ethical dilemma and moral distress that, due to the challenging behaviour of some prisoners, are common among prison nurses and can compromise ethical principles leading to emotional strain (Sasso et al, 2016). The emotional labour involved in caring for prisoners, coupled with the prioritisation of security over healthcare, contributes to the unique stressors experienced by nurses in prison settings (Goddard et al, 2019).
Box 2. Ethical dilemma and moral distress
- Ethical dilemma – a situation in which health professionals are faced with conflicting moral principles that can lead to competing values in decision making and, consequently, disagreements about treatment or the unfavourable alternative (Haahr et al, 2019)
- Moral distress – when healthcare providers know the ethically correct action to
take, but are constrained from acting on it due to various internal or external factors (Giannetta et al, 2021)
Addressing health inequalities
There are several ways in which nurses can aim to address health inequalities among people who are incarcerated, and work towards facilitating a health-promoting prison environment. First and foremost is the need for wider recognition of the specialist role of the nurse in custodial health, as well as training to provide trauma-informed care. Prison and custody nurses also play a key role in improving access to telehealth and promoting peer education – both of which are recognised as strategies to enhance healthcare delivery in custodial settings (Edge et al, 2019).
The role of learning disability nurses should also be highlighted as essential in this environment; as previously stated, almost a third of the prison population is thought to have learning disabilities (Prison Reform Trust, 2023). Learning disability nurses have enhanced communication and de-escalation skills, which are particularly beneficial in this setting, and they provide appropriate support to ensure healthcare needs are met for this vulnerable group (Trueland, 2020).
Recognition of the specialist role
Recognising custodial health nursing as a speciality is crucial for several reasons. Historically, custodial health has often been overlooked, with limited acknowledgement of the significant contributions made by custodial health nurses to the health and wellbeing of incarcerated populations (Burton, 2022). Therefore, establishing custodial health nursing as a specialty highlights the need for tailored educational programmes and professional development opportunities that are designed to address the unique demands of providing healthcare in prison settings (Burton, 2022).
Staff training
Improved health education, appropriate staffing and standardised training are highlighted as possible solutions to reduce health inequalities. These measures can encourage health screening, improve drug education and increase staff members’ ability to look for signs of ill health, which contribute to more equitable healthcare being provided in prisons (Arif, 2018). Goddard et al (2019) agreed, suggesting that educating custodial staff engages them and ensures parity across the prison system, reduces burnout and promotes wellbeing among prison nurses.
Specialised training and certification in custodial health nursing can enhance the competency and commitment of nursing professionals in this setting, leading to improved patient outcomes and a more skilled nursing workforce (Goddard et al 2019; Arif, 2018). By establishing custodial health nursing as a distinct field of practice and highlighting the contributions of custodial health nurses, this can promote advancements in education, research, professional development and excellence in patient care (Burton, 2022).
Trauma-informed care
Trauma-informed care is an approach that recognises the widespread impact of trauma and emphasises the importance of creating an environment that promotes healing and prevents re-traumatisation (Vaswani and Paul, 2019). This type of training is particularly crucial for nurses working in prisons due to the high prevalence of trauma among incarcerated individuals, stemming from various sources such as childhood abuse, violence and substance use (Vilhjalmsdottir et al, 2023).
Training in trauma-informed care equips nurses with the knowledge and skills needed to understand the effects of trauma on individuals’ mental health and behaviour. It enables nurses to recognise signs of trauma, respond empathetically and provide appropriate care that considers the individual’s past experiences (Vilhjalmsdottir et al, 2023). Furthermore, it can empower nurses to address the complex needs of individuals with a history of trauma, including mental health issues, substance abuse and self-harm behaviours (Vaswani and Paul, 2019).
By integrating trauma-informed care principles into their practice, nurses can establish a therapeutic rapport with patients, enhance communication and create a safe, supportive environment in the challenging context of a prison (Vaswani and Paul, 2019).
Telehealth
Telehealth services enhance healthcare accessibility by enabling remote consultations through telecommunications technology; access to them is crucial in prison settings (Senanayake et al, 2018). Telehealth has been shown to improve medical care for incarcerated individuals by addressing some of the challenges prisoners face, such as limited transportation, security issues and a shortage of health professionals in correctional facilities, as well as enabling prompt and essential healthcare delivery (Senanayake et al, 2018).
Improved communication between clinicians and prison patients facilitates access to specialist health services and contributes to better health outcomes, early detection of medical issues and continuity of care (Gajarawala and Pelkowski, 2021). Telehealth can also support mental health care and chronic disease management (Senanayake et al, 2018); in addition, it offers cost savings, increases healthcare delivery efficiency through potentially remote diagnoses, monitoring and treatment, thereby reducing in-person visits and optimising resources (Gajarawala and Pelkowski, 2021).
Telehealth also supports public health management by helping to control infectious diseases, mental health conditions and chronic illnesses among incarcerated populations (Edge et al, 2019). Furthermore, it helps maintain continuity of care for individuals transitioning from prison to the community, promoting better post-release health outcomes (Senanayake et al, 2018).
Advocating for improved access to telehealth is one approach nurses can take to improve health outcomes for prisoners.
Peer education programmes
Peer education programmes involve trained inmates delivering health education, support and interventions to their peers, and have proved to be acceptable, effective and empowering for both educators and recipients (Bagnall et al, 2015). By leveraging the unique position of peers, they can improve health knowledge, change behaviours and enhance overall health outcomes among incarcerated individuals.
A valuable component of prison health services, peer-based interventions are addressing issues such as substance abuse, infectious diseases and mental health concerns (South et al, 2017). In 2015, Bagnall et al reported that they had been found to be cost effective, feasible and valuable at identifying and addressing health and wellbeing concerns, while also having a positive effect on inmates’ health behaviours and wellbeing. They have also been shown to improve attitudes, knowledge and behaviours related to sexual health and HIV prevention (South et al, 2017).
Conclusion
There are clear disparities and inequalities in healthcare and wellbeing provision, both in the prison service and between prisons. These inequalities are compounded by the persistent stigmatisation of prisoners, and influenced by the many shifts of ownership and systematic variations of healthcare provision and delivery in the prison service. Contributing factors include environmental constraints, inconsistent implementation of healthcare models, poor communication, ad-hoc care, as well as education and staffing issues.
Although there are promising approaches that support opportunities to ensure excellent healthcare, these are not apparent across the whole of the UK prison estate. These differences present barriers to the safety of prisoners and have emphasised the pivotal role of nurses and MDTs in delivering high-quality care in this setting.
Specific challenges for nurses, such as moral distress, also need to be acknowledged and addressed. Improving prison healthcare requires staff training and education to enable a more inclusive and safer environment, appropriate staffing levels and a shift from reactive to continuous, coordinated care. NT
- Article 4 in the series looks at addressing ageism in healthcare.
Key points
- Prisoners are more likely to experience long-term conditions and poor mental health than the general population
- Environmental factors and poor communication can hinder access to effective healthcare in a prison setting
- Nurses are central to advocating for prisoners so they receive person-centred, trauma-informed care
- Standardised staff training and wider recognition of prison nursing as a specialty are needed
Arif T (2018) Hepatitis service provision at HMP Birmingham: progressing a previous service improvement plan. BMJ Open Quality; 7: 4, e000192.
Avieli H (2023) Prisoners’ experience of health self-management: a qualitative study. Journal of Nursing Scholarship; 55: 5, 926-935.
Bagnall A-M et al (2015) A systematic review of the effectiveness and cost-effectiveness of peer education and peer support in prisons. BMC Public Health; 15: 290.
Burton J (2023) The emergence of custodial health nursing as a specialty whose time has come: an Australian experience. International Nursing Review; 70: 3, 273-278.
Edge C et al (2019) Improving care quality with prison telemedicine: the effects of context and multiplicity on successful implementation and use. Journal of Telemedicine and Telecare; 27: 6, 325-342.
Gajarawala SN, Pelkowski JN (2021) Telehealth benefits and barriers. The Journal for Nurse Practitioners; 17: 2, 218-221.
Gaston S et al (2022) Correctional nurse education and training to care for and support prisoners with dementia: a systematic review of text and opinion. JBI Evidence Synthesis; 20: 5, 1275-1323.
Giannetta N et al (2021) Levels of moral distress among health care professionals working in hospital and community settings: a cross sectional study. Healthcare; 9: 12, 1673.
Goddard D et al (2019) Prison nurses’ professional identity. Journal of Forensic Nursing; 15: 3, 163-171.
Guttridge H et al (2024) Addressing challenges in the management of long-term conditions in prisons. journals.rcni.com, 9 May (accessed 5 August 2025).
Haahr A et al (2019) Nurses experiences of ethical dilemmas: a review. Nursing Ethics; 27: 1, 258-272.
Health Services Safety Investigations Body (2019) Management of chronic health conditions in prisons. hssib.org.uk, 10 October (accessed 5 August 2025).
House of Commons Health and Social Care Committee (2018) Prison Health. Twelfth Report of Session 2017-19. House of Commons.
Ismail N, de Viggiani N (2018) Challenges for prison governors and staff in implementing the Healthy Prisons Agenda in English prisons. Public Health; 162, 91-97.
Matheson FI et al (2022) Intellectual/developmental disabilities among people incarcerated in federal correctional facilities in Ontario, Canada: examining prevalence, health and correctional characteristics. Journal of Applied Research in Intellectual Disabilities; 35: 3, 900-909.
Ministry of Justice and HM Prison and Probation Service (2024) Prison Safety Policy Framework. MoJ and HMPPS.
National Institute for Health and Care Excellence (2016) Physical health of people in prison. nice.org.uk (accessed 4 July 2025).
NHS England (no date) RECONNECT. england.nhs.uk (accessed 5 August 2025).
NHS England (2023) A national framework for NHS: action on inclusion health. england.nhs.uk, 26 October 2023 (accessed 5 August 2025).
Nursing and Midwifery Council (2018) The Code. Professional Standards of Practice and Behaviour for Nurses, Midwives and Nursing Associates. NMC.
Prison Reform Trust (2025) Bromley Briefings Prison Factfile: February 2025. prisonreformtrust.org.uk (accessed 5 August 2025).
Prison Reform Trust (2023) Prison: The Facts. Bromley Briefings Summer 2023. PRT.
Prisons and Probation Ombudsman (2022) Former Ombudsman Sue McAllister publishes
final 2021/22 Annual Report. archive.ppo.gov.uk, 19 October (accessed 6 August 2025).
Rippon D et al (2021) The sources of adversity in the delivery of mental healthcare in prisons. Wellbeing, Space and Society; 2: 100046.
Sasso L et al (2016) Ethical issues of prison nursing: a qualitative study in Northern Italy. Nursing Ethics; 25: 3, 393-409.
Scottish Government (2022) Prison population: physical health care needs. gov.scot, 20 September (accessed 5 August 2025).
Senanayake B et al (2018) Telemedicine in the correctional setting: a scoping review. Journal of Telemedicine and Telecare; 24: 10, 669-675.
South J et al (2017) Developing a typology for peer education and peer support delivered by prisoners. Journal of Correctional Health Care; 23: 2, 214-229.
Toledanes YD et al (2021) The impact of quality improvement measures in the management of asthma patients in juvenile detention facilities. Cureus; 13: 2, e13351.
Trueland J (2020) Making reasonable adjustments in prisons: the role of the learning disability nurse. Learning Disability Practice; 23: 5, 7-10.
Vandergrift LA, Christopher PP (2021) Do prisoners trust the healthcare system? Health & Justice; 9: 15.
Vaswani N, Paul S (2019) ‘It’s knowing the right things to say and do’: challenges and opportunities for trauma-informed practice in the prison context. The Howard Journal of Crime and Justice; 58: 4, 513-534.
Vilhjalmsdottir A et al (2023) Women’s lived experience of the interconnectedness of trauma, substance use, and prison. Journal of Forensic Nursing; 19:1, 3-11.
Williams E et al (2022) What are health inequalities? kingsfund.org.uk, 17 June (accessed 5 August 2025).
Wright NMJ et al (2021) Long-term condition management for prisoners: improving the processes between community and prison. BMC Family Practice; 22: 80.
Help Nursing Times improve
Help us better understand how you use our clinical articles, what you think about them and how you would improve them. Please complete our short survey.
link




