
Determining the influence of an intervention of stress management on medical students’ levels of psychophysiological stress: the protocol of the PROMESS-Stress clinical trial | BMC Medical Education

Design and setting
This study is part of a larger randomized controlled trial assessing the effects of a multi-modal health intervention called the PROMESS project. The project will be presented to all 4th and 5th years undergraduate students of the Lyon-Est Faculty of Medicine (Claude Bernard University Lyon 1, France) through a lecture, and an informative email will be sent to their university addresses. Volunteer students will be able to register for the project by replying to the email. Participation in the project is seen as a reward, as students are expected to improve their ability to succeed in their studies. No monetary compensation is planned, as we aim to recruit only students who are intrinsically motivated to participate. The first 70 volunteers will be recruited. No exclusion criteria will be applied. For the entire PROMESS project, the 70 undergraduate medical students recruited will be randomized into two groups (1:2 ratio): a control group (n = 25) and an interventional group (n = 45) (stratified by gender and years of study). The present clinical trial (PROMESS-Stress) will specifically focus on the interventional group, in which 45 students will undergo a preventive program focused on stress management (Fig. 1).

Study Design. Seventy undergraduate medical students will be enrolled. First, they will perform baseline measurements. Then, they will be randomized into a control or an interventional group. This clinical trial (PROMESS-Stress) will specifically focus on the interventional group (n = 45). Each student in this group will be simply randomly assigned to one of the three periods (Period 1, Period 2, or Period 3) to follow a stress management program (i.e., PROMESS-Stress). This program will consist in three sessions, spaced 14 to 21 days apart. The primary outcome will be the PSS scores (Session 1, Session 2, Session 3). Secondary outcomes will comprise the VAS scores, BCI scores, and HRV markers (Session 1, Session 2, Session 3). Exploratory outcomes will include the student’s level of satisfaction regarding the program and will determine the moderators of the program’s efficacy. Abbreviations: BCI, Brief Cope Inventory; BIG-5, Big-5 questionnaire; HRSI, Holmes and Rahe Stress Inventory; HRV, Heart Rate Variability; PSS, Perceived Stress Scale; VAS, Visual Analog Scale
Ethic statement
The research project was discussed and approved by the Dean of the faculty (GR), the Lyon University Health Department, and a sample of local medical students. All procedures will be performed in adherence to the Helsinki declaration [26]. Ethical approval from the Institutional Review Board of the Claude Bernard University Lyon 1 (CUMG, France) has been obtained (IRB 2023–07-04–02), and the study has been registered in ClinicalTrials.gov (NCT06295133). Modifications to the protocol that may impact the conduct of the study will require a formal amendment. The participants’ anonymity and confidentiality will be ensured and maintained according to laws and regulations. The principal investigator (SS) will provide oral and written information, and participants will provide a written consent prior to enrollment following a sufficient reflection time (Additional file 2).
Characterization of the population at baseline
Before the intervention, participating students will complete a brief demographic survey, providing information regarding their year of study, age, gender, height, weight, level of physical activity and sport practice, and health issues (e.g., smoking status, any medication use). They will have their level of stress assessed through several psychological and physiological variables (baseline scores).
Psychological variables
A set of the following questionnaires will be answered at baseline.
Holmes and Rahe Stress Inventory (HRSI)
The HRSI is a 43-item questionnaire that assesses the number of personal (e.g., divorce, death of close relatives, personal injury, or illness) and professional stressors (e.g., change in the workplace) met during the last years [27]; we will used a recent scale [28]. For each item a binary answer is given (Yes/No), each “yes” answer is associated with a number ranging from 11 to 110. A high score indicates that the individual has been confronted to more and/or worse stressors, which may expose him or her to a greater risk of deteriorating health. A cumulative score is calculated and can be classified as follows: low risk (< 150), medium risk (150 to 300), and high risk of health degradation (> 300).
Big-5 questionnaire (BIG-5)
The BIG-5 is a 45-item questionnaire that assesses personality traits [29, 30]. Answers are given using a 5-point Likert scale. Five personality traits are extracted from the answers: agreeableness, openness, consciousness, extraversion, and neuroticism. Each personality trait is rated from 1 to 5, a high score indicates a higher expression of the trait. Personality will not be reassessed, as no change in personality is expected during the program [31]. The French-validated version of the BIG-5 will be used which has good internal consistency (Cronbach’s alpha 0.79) [30].
Perceived Stress Scale (PSS)
The PSS is a 10-item questionnaire that assesses the level of stress during the last month (four weeks) [32, 33]. Answers are given using a 5-point Likert scale. A total score ranging from 0 (none) to 40 (extreme) is calculated, and can be classified as follows: low (0 to 13), moderate (14 to 26), and elevated stress (27 to 40). The French-validated version of the PSS will be used which has good internal consistency (Cronbach’s alpha 0.83) [33].
Brief Cope Inventory (BCI)
The BCI is a 28-item questionnaire that assesses the coping behavior, we used the situational format to assess the behavior engaged during the last month (four weeks) [34,35,36]. The 28 items are classified in 4 strategies of coping behavior: problem solving (e.g., planning, active coping), positive thinking (e.g., humor, acceptance, positive reframing), social support (e.g., emotional support, venting, religion), and avoidance (e.g., denial, behavioral disengagement, substance use). Answers are given using a 4-point Likert scale and each strategy is rated from 1 to 4, a high score indicates that the behavior was highly engaged. The French-validated version of the BCI will be used which has satisfactory internal consistency (Cronbach’s alpha coefficients ranged from 0.64 to 0.82 for the 4 strategies) [35].
Physiological variables
A set of the following physiological stress variables will be recorded at baseline while students will be seated in a calm environment. Each student will be equipped with an ear pulse sensor that will record the cardiac activity during at least 7 min (emWave® Pro Plus Coherence Training software, version 3.14.1. 12,087; HeartMath Institute, Boulder Creek, CA, USA).
Cardiac coherence
The instantaneous and the cumulative cardiac coherence scores will be assessed [37,38,39]. Higher cardiac coherence score reflects lower physiological stress level.
Additional analysis of cardiac records will be performed using Kubios HRV Standard 3.5.0 software to extract other heart rate variability (HRV) markers. Records will be analyzed in 5 min-long segments, a proxy of longer recordings [40, 41]. However, it must be considered that as the HRV system responds rapidly, it remains possible that these 5-min recordings during a session might be insufficient to extrapolate on long-term stress exposure.
RMSSD
Root Mean Square of Successive Differences in ms, quantifies short-term variations between successive heartbeats, reflecting parasympathetic nervous system activity.
SDNN
Standard Deviation of NN intervals, in which NN means normal to normal beats (i.e., removing abnormal or false beat) in ms, reflects the overall variability in the time intervals between successive heartbeats.
pNN50%
NN50 is the number of pairs of successive intervals that differ by more than 50 ms. pNN50 is the percentage of NN50 over all NN intervals in a sample.
Low frequency (LF), High frequency (HF), and LF/HF ratio
HRV frequency-domain metrics calculate the spectral distribution of signal energy. HF represents the power spectral density (in ms2) of activity in the 0.15–0.40 Hz range, primarily linked to parasympathetic nervous system activity. LF represents the power spectral density of activity in the 0.04–0.15 Hz range, generally associated with sympathetic nervous system activity. The LF/HF ratio is commonly used to indicate the balance between sympathetic and parasympathetic activity in the nervous system [40].
Intervention
The PROMESS-Stress program has been developed with inputs from medical students and health professionals to prioritize participants’ well-being (i.e., previous co-construction workshop) [3] (Additional file 3). These participants identified the 4th and 5th years as the most suitable times to implement the program. They noted that students earlier in their studies may not yet be mature enough to fully appreciate the importance of maintaining a good quality of life or managing stressful situations. Conversely, implementing the program later in their studies was considered too close to the ranking exam and/or too late to be helpful for the challenges of residency. It was agreed that students will receive printed information about local health resources, accompanied by a reassuring discussion aimed at destigmatizing mental health issues during the program. Additionally, PROMESS-Stress experts may consult the Director of the University Health Service (AH) for advice on managing specific difficult situations.
The PROMESS-Stress program will consist of three sessions, spaced 14 to 21 days apart. A minimum of 5 weeks would separate the baseline from the third session. These sessions will be conducted in three distinct periods, with fifteen different medical students that will simply randomly undergo their sessions in one of the three periods. As such, the minimum duration of the procedure is 4 months. Each session will involve an individual meeting between a PROMESS-Stress expert and a student.
Expert training
According to the findings of the previous co-construction workshop [3], meetings will be conducted by graduate medical students, considered as experienced peers regarding their advancement in the medical curriculum (Additional file 3). Graduated medical students are well-acquainted with the curriculum’s constraints and have encountered similar stressful situations. In addition, they have experience in patient care and should possess the necessary skills to facilitate sessions, lead discussions on key issues, and identify primary concerns.
Prior to engaging in the sessions with students, those experienced peers will undergo a thorough training to be considered as experts. This training will involve several key steps, including reading a set of articles outlined in Additional file 4, observing each session at least once to obtain practical insights, and conducting themselves each session at least once, guided by an expert with theoretical and practical experience in stress management (SS). The observation and guidance steps will be repeated if necessary. This comprehensive training process, which might last approximately 4 days, is designed to ensure that peers will be adequately prepared and proficient to effectively deliver the PROMESS-Stress program. Graduated medical students who voluntarily become experts are expected to gain several benefits from their participation. First, they can realize their medical thesis on this project and receive close support from the scientific team. Second, they will develop valuable skills to assist future patients with stress-related disorders.
Overall organization of the sessions
Each session will consist of an individual meeting between a PROMESS-Stress expert and an undergraduate medical student (Fig. 2). To improve the reproducibility of the program, experts will follow a detailed step-by-step descriptive procedure for each session. Researchers will ensure that the program runs smoothly and that the experts have everything needed to conduct the sessions.

The PROMESS-Stress program. Prior to the program, the students will have their baseline level of stress assessed through several psychological and physiological variables. The PROMESS-Stress program will comprise three sessions, spaced 14 to 21 days apart. Each session will involve an individual meeting between a PROMESS-Stress expert and a student. The aim of these sessions is to identify the students’ needs regarding stress management in order to set individual goals, help them to reduce their stress level, and improve their coping skills. Between each session the student will fill a stress diary. Abbreviations: BCI, Brief Cope Inventory; HRV, Heart Rate Variability; PSS, Perceived Stress Scale; S1, Session 1; S2, Session 2
All sessions will follow a similar structure. The session will start with a short introduction talk, in which the expert will briefly explain the main steps of the session. Following this, a 7-min cardiac recording will be conducted, during which the student will be asked to complete questionnaires. The expert will then provide pedagogical content about stress and coping, introducing key principles of well-established coping interventions. During the meeting, the student will be provided the possibility to discuss his/her own source of stress and coping mechanisms, allowing both the student and the expert to identify the student’s needs regarding stress management. Finally, specific advice and goals will be set based on this discussion, partly based on a predefined list created for medical students in the prior co-construction workshop (Additional file 5) [3]. Individual diagnostics related to stress and coping, along with self-monitoring tools, will be provided to help students eliminate unhealthy habits and raise awareness and/or reinforce healthier ones.
Questionnaires
At the beginning of each session, the student will complete the PSS and BCI questionnaires, and will answer several 100-mm Visual Analog Scales (VAS). Each VAS will prompt the student to move a cursor to indicate his/her response. The cursor will start at the 0 position for each question [5, 42].
VAS – stressors quantity
The quantity of stressors encountered by the student will be assessed on a VAS asking “In the past two weeks, how many stressful situations have you encountered?” ranging from 0 (maximum/extreme) to 100 (zero).
VAS – stress quantity
The student’s level of stress will be assessed on a VAS asking “In the past two weeks, how would you characterize your stress level?” ranging from 0 (maximum stress) to 100 (no stress at all).
VAS – stress quality
The emotional valence associated with the student’s stress level will be assessed on a VAS asking “Over the past two weeks, how would you characterize your stress?” ranging from 0 (very negative feeling) to 100 (very positive feeling).
VAS – stress coping
The student’s management of stressful situations will be assessed on a VAS asking “Over the past two weeks, how have you managed stressful situations?” ranging from 0 (very bad stress coping) to 100 (excellent stress coping).
Session description
Session 1
The first session will last approximately 60 min (Fig. 2). This session will begin with a brief presentation of the expert’s background as well as with an explanation regarding the confidentiality of the exchanges. Then the following points will be addressed:
-
Assessment of psychophysiological stress level. The student will answer the PSS, BCI, and VAS. Simultaneously, a 7-min cardiac recording will be conducted in a seated position using the ear pulse sensor.
-
Pedagogical content. This content is composed of 3 main sections. The first one provides information on a stress cycle containing both theoretical background on stress and individual data (Fig. 3A). It is composed of 3 parts: (i) the “stressful events” part with the quantity of stressors encountered by the student (HRSI baseline score); (ii) the “coping” part with the coping definition (i.e., conscious or unconscious strategies/behaviors implemented to cope with stressful situations); and (iii) the “stress” part with the student stress level (PSS baseline score). By providing quantified information to the student, we allow the expert and the student the possibility to discuss these scores, and more importantly, to identify the origin of the student’s stress and his/her needs. The second part provides information on the overall stress response periods (i.e., anticipatory stress, acute stress, recovery) (Fig. 3B) [39]. The third one provides explanations on the most appropriate moments for the implementation of coping behaviors during the overall stress response (Fig. 3C) [39, 42]. Pedagogical content also provides theoretical information on physiological stress markers (HRV) and introduces well-established coping interventions, mindfulness, relaxing breathing and cardiac biofeedback. Coping interventions are empirically supported methods shown to be effective in reducing psychological and physiological stress. For example, a recent meta-analysis [17] concluded that mindfulness-based interventions effectively reduce subjective stress in medical students, both in the short and long term. Similarly, a study by Sperling [20] confirms that, despite a wide variety of mindfulness interventions offered to medical students worldwide, they produce an overall small to moderate effect on stress reduction. Others studies repeatedly support the efficacy of relaxing breathing and cardiac biofeedback interventions [18, 21, 22, 24, 39].

Examples of a pedagogical content of the PROMESS-Stress program. During the sessions, students will be provided with theoretical information on stress and coping (i.e., pedagogical content). This figure illustrates some examples of the PROMESS-Stress supports given during S1. A Stress cycle. B Overall stress response periods. The figure illustrates the period of reactivity and recovery that precedes and follows, respectively, a confrontation with a stressful event (i.e., acute stress). C Implementation of coping strategies; moments of implementation are illustrated in green. Figure adapted from Schlatter (2021) [39]. Abbreviations: HRSI, Holmes and Rahe Stress Inventory; PSS, Perceived Stress Scale
-
Cardiac biofeedback exercise. Then a cardiac biofeedback exercise will be performed using the ear pulse sensor connected to a computer via an USB. The emWave® interface displays real-time heart rate, continuous cardiac coherence score, and a breathing guide cursor (for more detailed procedure [39]). During the first two minutes of recording, the expert will present the interface and no specific breathing instruction will be given. The student will then engage in a 5-min paced breathing exercise at 6 breaths per minute, with the final two minutes dedicated to mentally visualizing an image that aligns with the breathing rhythm (e.g., a balloon inflating and deflating). Then, the recording will continue for another 2 min without instruction on breathing, nor visual on the interface. After the exercise, the individual cardiac coherence score will be provided to the student in order to raise his/her awareness regarding the physiological modification related to paced breathing. In addition, the student will be invited to download a free smartphone application for further self-training (RespiRelax + , © Les Thermes d’Allevard, version 2.2. 2023).
-
Stress diary. A stress diary will be given to the student (Fig. 4). The student will be instructed to fill it out until the next session, reporting any stressful situations he/she encounters on a daily basis. For each stressful situation, he/she will be asked to briefly describe it (in 3 or 4 words), estimate its duration, and rate its intensity on a scale ranging from 1 (minimum) to 5 (maximum). In addition, he/she will indicate whether he/she had engaged in coping behaviors such as relaxing breathing, mindfulness, physical activity, positive thinking, or others. The expert and the student will fill the present day of the diary together to provide an example.
Fig. 4 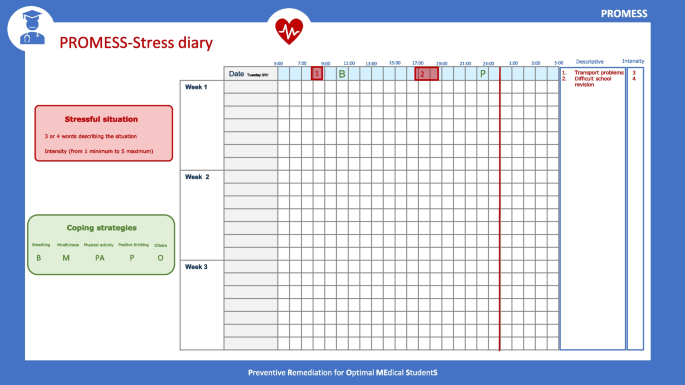
PROMESS-Stress diary. Between the sessions, students will fill this diary, reporting any stressful situations they encounter (red part) and the coping behavior they have engaged (green part) on a daily basis. For each stressful situation, he/she will be asked to briefly describe it (in 3 or 4 words), estimate its duration, and rate its intensity on a scale ranging from 1 (minimum) to 5 (maximum). In addition, he/she will indicate whether he/she had engaged in coping behaviors such as relaxing breathing, mindfulness, physical activity, positive thinking, or others, by writing a letter to specify which coping methods were used. Abbreviations: B, relaxing breathing; M, Mindfulness; PA, Physical activity; P, positive thinking; O, Others
-
Advice. During the entire session, advice concerning regular and situation-specific coping behaviors will be provided. Advice will be based on the predetermined list (Additional file 5) [3].
-
Goals. At the end of the session, the expert will answer all the questions that may arise and will settle the student’s goal for the next session. Both the student and the expert will write the goals and will sign an agreement, which should promote the student’s commitment and motivation [3].

At the end of each session, the expert will report the following information:
-
Likert – Expert comfort. The expert will have to report his/her level of comfort regarding his/her relationship with the student during the session on a 5-point Likert scale (1: not comfortable at all, 2: slightly comfortable, 3: fairly comfortable, 4: comfortable, 5: very comfortable).
-
Likert – Expert satisfaction. The expert will have to report his/her level of satisfaction regarding his/her animation of the session on a 5-point Likert scale (1: not satisfied at all, 2: slightly satisfied, 3: fairly satisfied, 4: satisfied, 5: very satisfied).
-
Likert – Advice given. For each predefined advice (Additional file 5), expert will report on a 5-point Likert scale if he/she: 1) did not mention this during the meeting; 2) mentioned this but did not directly advise it; 3) mentioned this and recommended it; 4) had set this in the goals; 5) performed a positive reinforcement. He/she will also report any advice that has been given during the session that may not be present in the predefined list.
Session 2
The second session will last approximately 60 min, the following points will be addressed (Fig. 2):
-
Assessment of psychophysiological stress level. Using the same procedure as described above.
-
Feedback on stress diary. The stress diary filled out between S1 and S2 will be discussed. The expert will question the student regarding the stressful situations encountered and the types of coping engaged. The expert will also assist the student in retrospectively identifying both of them. This is an important part of the session, enabling the expert to detect common stressful situations. The expert will identify whether some stressors can be anticipated and may benefit from specific (anticipated) or recovery coping strategies. The declaration of coping behaviors is crucial, as it allows the student to recognize which engaged actions are associated with stress reduction. Personal techniques will be discussed and may be further advised by the expert.
-
Feedback on S1 goals. A discussion between the expert and the student will help to identify the obstacles and facilitators to achieve each previously established goal.
-
Pedagogical content. A brief reminder regarding the stress cycle, the overall stress response and the appropriate moments to implement coping behaviors will be provided (Fig. 3).
-
Personality. The student will first receive information regarding personality construction, focusing on five traits: agreeableness, openness, conscientiousness, extraversion, and neuroticism [29, 30]. Subsequently, he/she will learn about the links between each personality trait and the level of vulnerability to stress, based on previous findings [43], particularly those concerning medical students [22, 24]. The student will then receive his/her personality trait scores (BIG-5 baseline scores), giving insights into his/her propensity for stress vulnerability.
-
Coping. The student will first receive information on coping behaviors, four main strategies of behaviors will be discussed: problem solving, positive thinking, social support, and avoidance [34, 35]. Subsequently, he/she will learn about the links between each strategy and stress vulnerability based on previous findings in medical students [5]. He/she will then receive his/her coping behavior (BCI baseline scores), giving insights into his/her propensity for stress vulnerability.
-
Cardiac biofeedback exercise. The student will perform the following exercise to estimate his/her resonant breathing frequency using an adapted version of the Lehrer procedure [40, 44, 45]. First, the expert will briefly explain the emWave® interface again for 1 min. Following this, the student will engage in 2-min of paced breathing set at 6 breaths per minute, followed by a 1-min break during which he/she can choose to explore a faster or slower breathing frequency. Then the student will perform a 2-min breathing exercise with the chosen modified pace, followed by an additional 1-min break. The expert will identify the most effective breathing frequency to reach a high and sustainable cardiac coherence (this should be close to the student’s breathing resonance). The student will finally be advised to practice at this frequency for further self-training.
As performed in S1, advice will be provided throughout the entire session. The student will receive a new stress diary to be filled until the next session. The expert will address all questions and individual goals will be established and signed.
Following the meeting, the expert will report his/her level of comfort and satisfaction, rate the predefined advice, and report all the goals established during this session. In addition, the expert will estimate whether the student has achieved the goals previously set (S1 goals) on a 4-point Likert scale (i.e. 0: not achieved at all, 1: slightly achieved, 2: fairly well achieved, 3: well achieved).
Session 3
The third session will last approximately 45 min, the following points will be addressed (Fig. 3):
-
Assessment of psychophysiological stress level. Using the same procedure as described above.
-
Feedback on stress diary. The stress diary filled out between S2 and S3 will be discussed as described above.
-
Feedback on S2 goals. Feedback on S2 goals will be provided as described above.
-
Feedback on achievements. To offer the student a comprehensive overview of his/her achievements across the program, the expert will provide an individualized printed summary that will comprise: 1) cardiac coherence scores during the cardiac biofeedback exercise (S2) to remind the physiological impact of paced breathing; 2) the goals set in previous sessions (S1, S2) and the BCI and PSS scores (baseline, S1, S2, S3) to raise discussion and awareness regarding the student’s progress. Progression will be discussed based on the goals in order to help the student to identify what was effective for him/her. In addition, the student will be encouraged to proactively determine and report his/her long-term goals (S3 goals) on his/her own, to enhance autonomy, short- and long-term commitment, as well as motivation.
As performed in S1 and S2, advice will be provided throughout the entire session and the expert will address all questions. Then, a printed support with local health resources information and the comprehensive list of advice (Additional file 5) will be distributed to help the student adopt long-term changes and provide opportunities to find advice that matches his/her future needs.
Just before ending the session, the level of student satisfaction regarding the PROMESS-Stress program will be assessed through several 100-mm VAS. Each VAS will prompt the student to move a cursor to indicate his/her response. The cursor will start at the 0 position for each question.
-
Composite score – Student’s satisfaction. The satisfaction will be measured using a composite score. It will be the mean of two sub-scores: 1) the specific score (stress and coping): mean of the score obtained at the VAS: “Do you think the intervention has helped you to lower your stress level?” and at the VAS: “Do you think the intervention allowed you to better manage the stressful events you have encountered?”, 2) the general score (relevance and sustainability): mean of the score obtained at VAS: “Do you think the proposed goals were suitable for your daily life?” and at the VAS: “Do you think you can sustain the performed changes in habits?”. All VAS score ranging from 0 (absolutely not) to 100 (completely). For all scores of student’s satisfactions, a score lower than 30 will be considered as highly negative, a score ranging from 30 to 44 as negative, a score from 45 to 54 as neutral, a score from 55 to 69 as positive, and a score equal or superior to 70 as highly positive.
At the end of this session, the expert will report his/her level of comfort and satisfaction, rate the predefined advice, report all the goals settled, and estimate whether the student has achieved the goals settled in S2. He/she will report his/her overall level of satisfaction regarding the student’s progress during the PROMESS-Stress program (“Are you satisfied with the student’s progress during the whole intervention?”) on a Likert scale ranging from 1 (not satisfied at all) to 5 (very satisfied).
Availability of the PROMESS-Stress material
All materials necessary to perform the PROMESS-Stress program are available from the authors upon reasonable request (SS, AM, [email protected] and/or personal mail).
Data management and monitoring
The principal investigator (SS) will ensure that the protocol and ethical guidelines for data collection and analysis will be followed. She will be responsible for maintaining the anonymity of the included students (participants will be assigned a unique identification code). In addition, the students will receive a letter with information which clarifies how their data will be used regarding the General Data Protection Regulation (GDRP), including the contact details of the university’s data protection officer, as well as the contact of the principal investigator. Students will be informed that if they wish to withdraw their data, they have to contact the principal investigator who will conduct a dropout analysis. All source documents, including written consent and printed materials from the sessions, will be stored in a secure locker at the RESHAPE Laboratory (INSERM U1290, Université Claude Bernard Lyon 1, Lyon, France) for a five-year period after the last publication of results. Raw data, processed data, and analysis scripts will be stored on a password-protected computer at the RESHAPE laboratory, accessible only to registered investigators (SS, AM). The database preparation and statistical analysis will be conducted anonymously. Since the study involves minimal risk to participants, a Data Monitoring Committee (DMC) was deemed unnecessary; moreover, the project was approved by an institutional review board (IRB: 2023–07-04–02), affirming adequate monitoring. No spontaneously reported adverse events and other are expected.
Data analysis
Data analysis will take place once all data have been collected. No interim analyses and stopping guidelines to terminate the study are planned.
Data analyzed
Variables will be expressed as means with standard deviations and ranges, medians with interquartile ranges, or counts and percentages. Data will be analyzed according to the intention-to-treat principle and presented in accordance with international Consolidated Standards of Reporting Trials guidelines. A p-value < 0.05 will be considered statistically significant, while p < 0.10 will be a trend. All models’ assumptions will be checked. For linear regressions, the β coefficients with their 95% confidence interval and the adjusted coefficients R2 will be provided. Mean imputation will be performed, replacing missing values with the mean of other questions addressing the same categories of the questionnaire. This approach allows us to retain as much data as possible for our analyses. All statistical analysis will be performed using the most recent version of the R software [46].
Outcomes
The primary outcome will be the PSS (scores obtained at S1, S2, S3). The secondary outcomes will be other psychophysiological stress variables (scores obtained at S1, S2, and S3; Table 1). The outcomes will be assessed by the PROMESS-Stress experts.
Hierarchical ordering
An a priori hierarchical ordering of secondary outcomes has been performed (Table 1). The ordering has been defined by the PROMESS-Stress experts according to the existing literature, their expectations regarding the program, and the results of a pilot study [3]. This hierarchical ordering will allow us to draw conclusions on the impact of the program until the p-value becomes non-significant. In cases where the p-value will become non-significant, the following secondary outcomes will be assessed as exploratory outcomes [47].
A priori–sample size
The sample size was a priori calculated for the primary outcome (evolution of the PSS scores during the S1, S2, and S3). Based on an expected medium effect size for repeated measures (f = 0.20, α = 5%, power = 0.80, 3 measurements) the calculation resulted in a total sample size of 42 participants (G*Power v3.1.9.6). To ensure robustness against potential attrition or loss of data, we will recruit an additional 10% of volunteers, resulting in a total sample size of 45 participants.
Statistical analysis plan
Primary and secondary outcomes
Linear mixed models (with a random effect for participants and experts) will be performed to explore the impact of the PROMESS-Stress program on the primary and the secondary outcomes following the hierarchical ordering. For the physiological secondary outcomes, models will be adjusted for age, gender, BMI, smoking status, and level of physical activity. Students who will report the use of beta-blockers at baseline will be excluded from HRV analysis.
Exploratory outcomes
Moderators of efficacy
The efficacy of the program will be determined by a delta score on PSS (score S3 – score S1); a negative delta score will express a reduction, a neutral score no change, and a positive score an increase in stress level during the program. As such, lower delta score will represent higher efficacy. A linear model will explore whether the delta score is influenced by the student’s characteristics such as gender, age, and study year, as well as by pre-existing vulnerabilities to stress at inclusion, as assessed by the baseline levels of stress and stressors (PSS and HRSI baseline scores). This model will also explore the influence of the periods (period 1, period 2, period 3) and the experts on the delta score.
Composite score – Student’s satisfaction
The student’s level of satisfaction regarding the PROMESS-Stress program will be determined; the mean composite score of satisfaction should be equal or greater than 70 to conclude that the students will be highly satisfied (one sample t-test or one-sample Wilcoxon signed-rank test). Similarly, the four scores of satisfactions will be independently explored, and compared to 70, in order to have a greater insight into the program’s acceptability.
Moderators of satisfaction
A linear model, will explore the influence of student’s characteristics (gender, age, study year), student’s pre-existing vulnerabilities to stress (PSS and HRSI baseline scores), periods, and experts on the composite score of satisfaction.
Dissemination and open science strategies
This study adopts citizen science by co-constructing the research with medical students and health professionals, ensuring that the program reflects real-life needs and diverse perspectives. The study protocol has been pre-registered to enhance transparency and reduce biases. Anonymous data and analysis scripts will be made available to promote reproducibility. In order to ease the replication of the present protocol by other medical schools, all materials will be freely available upon request. Results will be published in open access journals to ensure broad accessibility and will be presented at international and national scientific congresses, in peer-reviewed scientific journals, in medical thesis dissertations, and in communications to local and national educational committees. Additionally, we will organize a one-day local congress to present the results and promote advances in medical education.
Preliminary survey on students’ interest
To determine the interest of medical students in the PROMESS program, a survey was administered in June 2023 to all the 535 fourth-year undergraduate medical students of the Lyon-Est Faculty of Medicine (Claude Bernard University Lyon 1, France). Students answered several questions, including: “How interested are you in following an intervention aiming to reduce stress?”. Ten percent of students were not interested at all, and 14% were not interested. Conversely, more than 75% were interested (30% moderately interested, 28% interested, and 18% very interested). Students also answered: “Would you be interested in the implementation of personal support within a stress management program?”. Twenty percent were not interested at all, and 16% were not interested. Conversely, more than 64% were interested (24% moderately interested, 25% interested, and 15% very interested). These preliminary results reinforce the pertinence and need for the PROMESS-Stress program.
link
:max_bytes(150000):strip_icc()/GettyImages-1353223720-6aa033a7c6414debbec9dbe02bdaeb63.jpg "What Is the Holmes and Rahe Stress Scale?")





